

Development, testing and comparison of novel lifestyle-based prediction models for risk of coronary heart disease
- PMID: 41120693
- PMCID: PMC12541051
- DOI: 10.1038/s41598-025-99536-1
Development, testing and comparison of novel lifestyle-based prediction models for risk of coronary heart disease
Abstract
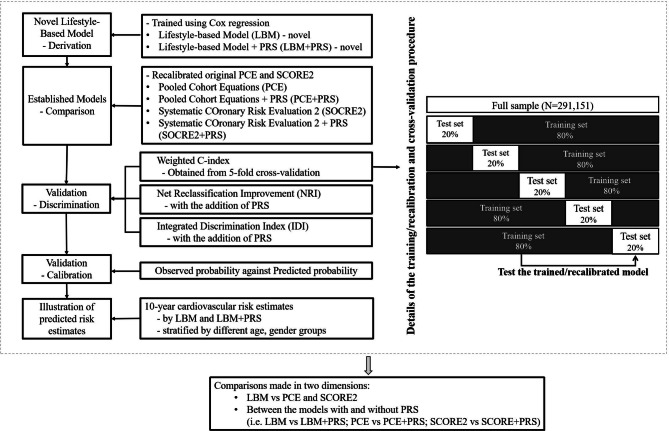
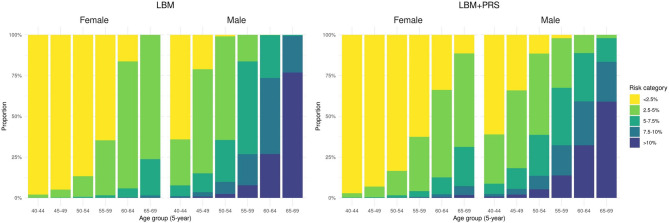
Prediction of coronary heart disease (CHD) risk through standard equations relying on laboratory-based clinical markers has proven challenging and needs advancement. This study aims to derive and cross-validate novel CHD-risk prediction models based on lifestyle behaviours including wearables and polygenic risk scores (PRS), with comparison to the established Pooled Cohort Equations (PCE) and Systematic COronary Risk Evaluation 2 (SCORE2). This study included 291,151 white British individuals of UK Biobank. Cox regression was applied to derive Lifestyle-Based Model (LBM) for CHD-risk prediction incorporating age, sex, body mass index, dietary intake score (0-3; derived from self-reported food types), smoking status, and physical activity (wearable-device-derived Euclidean Norm Minus One). Weighted PRS for CHD was calculated based on 300 genetic variants. Over a median 13.8-year follow-up, 13,063 CHD incidence cases were ascertained. The C-index (indicative of discrimination) of the LBM, PCE and SCORE2 was 0.713 (95% Confidence Interval [CI]: 0.703-0.722), 0.714 (95% CI: 0.705-0.724) and 0.709 (95% CI: 0.700-0.719). Adding PRS to LBM, PCE and SCORE2 increased the C-index to 0.733 (95% CI: 0.724-0.742), 0.726 (95% CI: 0.716-0.735) and 0.721 (95% CI: 0.711-0.730). The LBM with and without PRS both demonstrated good calibration, demonstrating by p-values of 0.997 and 0.999. The addition of PRS to LBM marginally improved calibration, with the slope increasing from 0.981 to 0.983. Integrating PRS rendered a positive categorical net reclassification improvement (cut-off point: 7.5%) of 4.30% for LBM. The non-laboratory-based LBM, integrating wearable-based and anthropometric data, demonstrated moderate cardiovascular risk prediction accuracy, though external validations remain to be explored.
Keywords: Coronary heart disease; Physical activity; Polygenic risk score; Risk prediction modelling; UK biobank.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: The UK Biobank was approved by the North-West Multi-Centre Research Ethics Committee (Ref: 11/NW/0382). The present study was approved by the Institutional Review Board of The University of Hong Kong/ Hospital Authority Hong Kong West Cluster (UW 21–542).
Figures



References
-
- Ntalla, I., Kanoni, S. & Zeng, L. Genetic risk score for coronary disease identifies predispositions to cardiovascular and noncardiovascular diseases. J. Am. Coll. Cardiol.73(23), 2932–2942 (2019).
-
- Barbaresko, J., Rienks, J. & Nöthlings, U. Lifestyle indices and cardiovascular disease risk: a meta-analysis. Am. J. Prev. Med.55(4), 555–564 (2018).
-
- Myers, R. H., Kiely, D. K., Cupples, L. A. & Kannel, W. B. Parental history is an independent risk factor for coronary artery disease: The Framingham Study. Am. Heart. J.120 (4), 963–969 (1990).
Publication types
MeSH terms
Grants and funding
- MC_UU_00006/1, MC_UU_00006/4 and MC_UU_12015/3/MRC_/Medical Research Council/United Kingdom
- MC_UU_00006/1, MC_UU_00006/4 and MC_UU_12015/3/MRC_/Medical Research Council/United Kingdom
- MC_UU_00006/1, MC_UU_00006/4 and MC_UU_12015/3/MRC_/Medical Research Council/United Kingdom
- IS-BRC-1215-20014/NIHR Cambridge Biomedical Research Centre
- IS-BRC-1215-20014/NIHR Cambridge Biomedical Research Centre
LinkOut - more resources
Full Text Sources
