

Fetal cardiac masses
- PMID: 41123646
- PMCID: PMC12594719
- DOI: 10.1007/s00247-025-06431-y
Fetal cardiac masses
Abstract
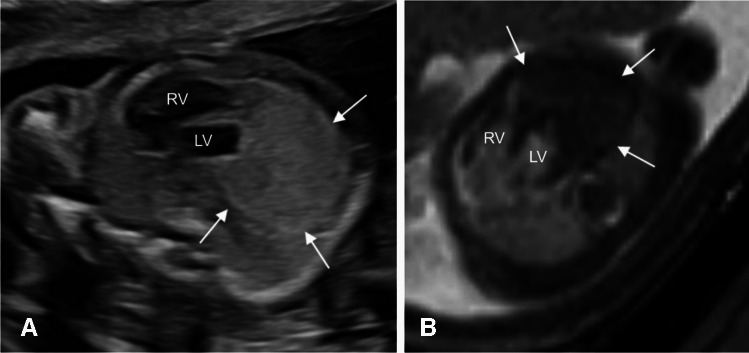
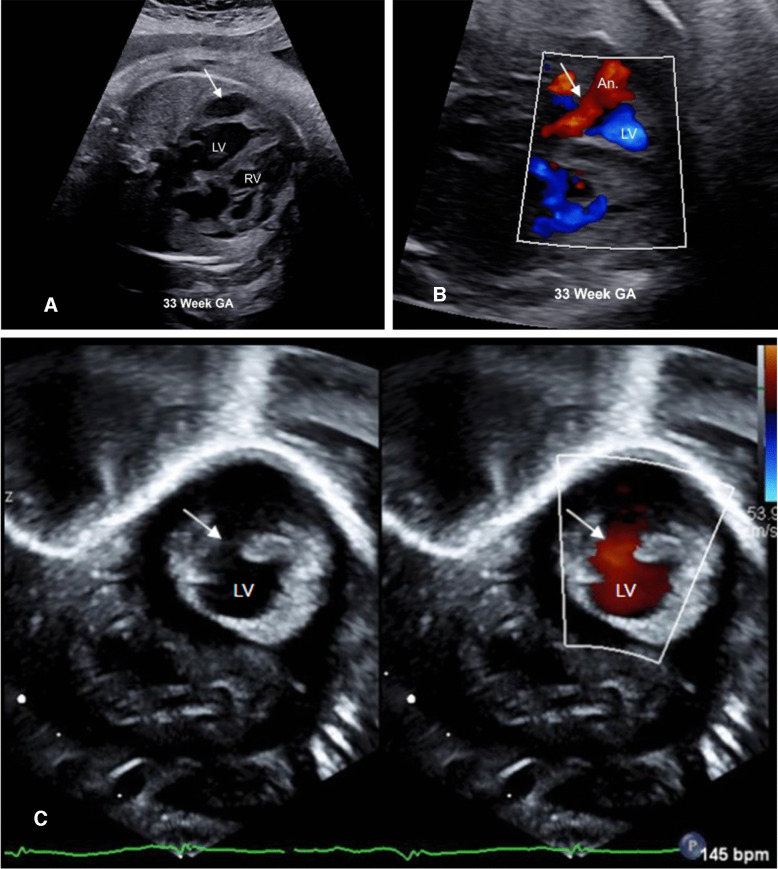
Although rare in the pediatric population, cardiac tumors represent a significant portion of prenatally detected masses, second only to sacrococcygeal teratomas. Fetal cardiac masses are predominantly benign, with rhabdomyoma being the most common fetal cardiac mass in the setting of tuberous sclerosis. Multiple lesions are pathognomonic for rhabdomyomas and prompt evaluation for tuberous sclerosis. Fibroma, teratoma, and hemangioma are other consistently detected cardiac tumors. In this article, we review the epidemiology, imaging, treatment, and outcomes of these fetal cardiac masses, emphasizing the role of imaging in surveillance, identifying complications, refining the differential diagnosis, and recognizing potential diagnostic pitfalls.
Keywords: Fetus; Fibroma; Heart neoplasms; Hemangioma; Rhabdomyoma; Teratoma.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: None
Figures





References
-
- Camargo FM, Brizot MdL, Francisco RPV, de Carvalho WB, Ikari NM, Peres SV, Lopes MAB, Lopes LM (2024) Resultados perinatais e seguimento em Longo prazo de tumores cardíacos fetais: Estudo de coorte histórica de 30 anos. Arq Bras Cardiol. Sociedade Brasileira de Cardiologia 121(1):e20220469 - PMC - PubMed
-
- Hornberger LK, McBrien A (2018) Fetal cardiac tumors. In: Yagel S, Silverman NH, Gembruch U (eds) Fetal cardiology: Embryology, genetics, physiology, echocardiographic evaluation, diagnosis, and perinatal management of cardiac diseases, 3rd edn. Philadelphia: CRC Press
-
- Kogon B, Shehata B, Katzenstein H, Samai C, Mahle W, Maher K, Olson T (2011) Primary congenital infantile fibrosarcoma of the heart: the first confirmed case. Ann Thorac Surg 91:1276–1280 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
