

Post-traumatic stress and genetic interactions affect tobacco and alcohol use after trauma: findings from a multi-ancestry cohort
- PMID: 41136357
- PMCID: PMC12552440
- DOI: 10.1038/s41398-025-03593-z
Post-traumatic stress and genetic interactions affect tobacco and alcohol use after trauma: findings from a multi-ancestry cohort
Abstract
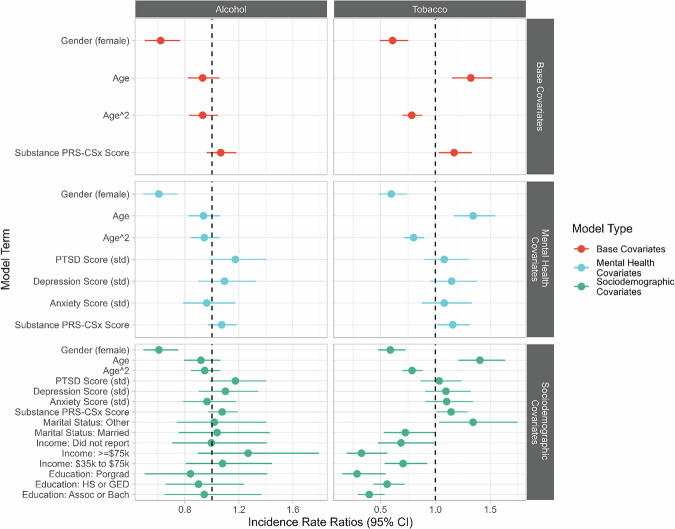
Tobacco smoking and drinking alcohol are common substance use behaviors influenced by both genetic risk and environmental exposures. Traumatic events are highly prevalent, affecting about 70% of people in their lifetime. After trauma, it is unclear what role post-traumatic stress disorder (PTSD) symptoms play in substance use behaviors when accounting for this genetic risk. We used data from the Advancing Understanding of RecOvery afteR traumA (AURORA), which included 2973 participants recruited at emergency departments (EDs) within 72 h of a traumatic event and followed over time. We measured PTSD symptoms via PTSD Checklist for the DSM-5. Tobacco and alcohol consumption as frequency, quantity, and quantity-frequency in the past 30 days. We generated polygenic risk scores with continuous shrinkage for cross-ancestry estimation (PRS-CSx). We tested for main effects between PRS-CSx scores and interactions with PTSD using quasipoisson regression, with week 8 PTSD symptoms and month 6 substance use behaviors after the traumatic event. Tobacco PRS-CSx score increased the risk of tobacco use by 14% (95% CI: 1.01, 1.29, p = 0.03), and alcohol PRS-CSx score did not demonstrate consistent associations in the whole cohort (IRR: 1.08, 95% CI: 0.97, 1.19, p = 0.16). When stratified by ancestry group, both tobacco (IRR: 1.36, 95% CI: 1.14, 1.61, p < 0.001) and alcohol (IRR: 1.24, 95% CI: 1.07, 1.44, p = 0.005) PRS-CSx scores were associated with their respective outcomes in the European ancestry subcohort. Participants with lower genetic risk had stronger associations between re-experiencing symptoms and tobacco use, while participants with higher genetic risk demonstrated weaker association between re-experiencing symptoms and tobacco use. A similar pattern was observed for negative alterations in cognition/mood (NACM) symptoms-participants with lower PRS-CSx scores had stronger associations between NACM symptoms with tobacco use, compared to participants with higher PRS-CSx scores. These interactions were both statistically significant, suggesting an antagonistic effect between PRS-CSx scores and PTSD symptoms on tobacco use.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Dr. Garrison-Desany has no competing interests related to this work, though received a contract from Indivior PLC from February to May 2025 for research unrelated to this manuscript. Dr. Hinojosa receives support from the National Institute of Alcohol Abuse and Alcoholism, K99AA031333. Dr. Neylan has received research support from NIH, VA, and Rainwater Charitable Foundation, and consulting income from Jazz Pharmaceuticals. In the last three years Dr Clifford has received research funding from the NSF, NIH and LifeBell AI, and unrestricted donations from AliveCor Inc, Amazon Research, the Center for Discovery, the Gates Foundation, Google, the Gordon and Betty Moore Foundation, MathWorks, Microsoft Research, Nextsense Inc, One Mind Foundation, and the Rett Research Foundation. Dr Clifford has financial interest in AliveCor Inc and Nextsense Inc. He also is the CTO of MindChild Medical with significant stock. These relationships are unconnected to the current work. Dr. Germine receives funding from the National Institute of Mental Health (R01 MH121617) and is on the board of the Many Brains Project. Her family also has equity in Intelerad Medical Systems, Inc. Dr. Rauch reported serving as secretary of the Society of Biological Psychiatry; serving as a board member of Community Psychiatry and Mindpath Health; serving as a board member of National Association of Behavioral Healthcare; serving as secretary and a board member for the Anxiety and Depression Association of America; serving as a board member of the National Network of Depression Centers; receiving royalties from Oxford University Press, American Psychiatric Publishing Inc, and Springer Publishing; and receiving personal fees from the Society of Biological Psychiatry, Community Psychiatry and Mindpath Health, and National Association of Behavioral Healthcare outside the submitted work. Dr. Jones has no competing interests related to this work, though he has been an investigator on studies funded by AstraZeneca, Vapotherm, Abbott, and Ophirex. Dr. Harte has no competing interest related to this work, though in the last three years he has received research funding from Aptinyx and Arbor Medical Innovations, and consulting payments from Memorial Sloan Kettering Cancer Center, Indiana University, The Ohio State University, and Dana Farber Cancer Institute. Dr. McLean has served as a consultant for Walter Reed Army Institute for Research, Arbor Medical Innovations, and BioXcel Therapeutics, Inc. Dr. Ressler has performed scientific consultation for Bioxcel, Bionomics, Acer, and Jazz Pharma; serves on Scientific Advisory Boards for Sage, Boehringer Ingelheim, Senseye, and the Brain Research Foundation, and he has received sponsored research support from Alto Neuroscience. Dr. Koenen’s has been a paid scientific consultant for the US Department of Justice and Covington Burling, LLP over the last three years. She receives royalties from Guilford Press and Oxford University Press.
Figures



References
-
- Brady KT, McCauley JL, Back SE The comorbidity of Post-traumatic Stress Disorder (PTSD) and substance use disorders. In: el-Guebaly N, Carrà G, Galanter M, Baldacchino AM (eds). Textbook of addiction treatment: international perspectives. Cham: Springer International Publishing; 2021, pp 1327-39.
MeSH terms
Grants and funding
- K99 AA031333/AA/NIAAA NIH HHS/United States
- U01 MH110925/MH/NIMH NIH HHS/United States
- U01MH110925/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- K99AA031333/U.S. Department of Health & Human Services | NIH | National Institute on Alcohol Abuse and Alcoholism (NIAAA)
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
