

Coronary Bifurcation PCI-Part I: Fundamentals
- PMID: 41149281
- PMCID: PMC12565571
- DOI: 10.3390/jcdd12100410
Coronary Bifurcation PCI-Part I: Fundamentals
Abstract
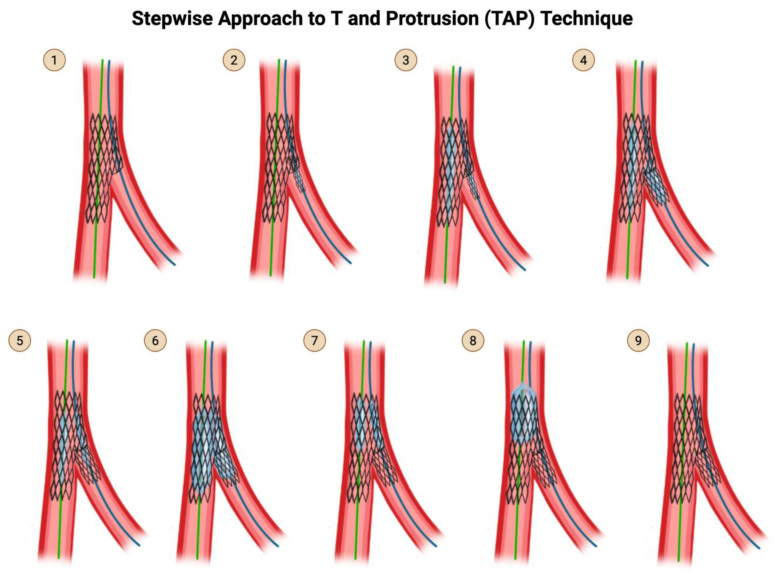
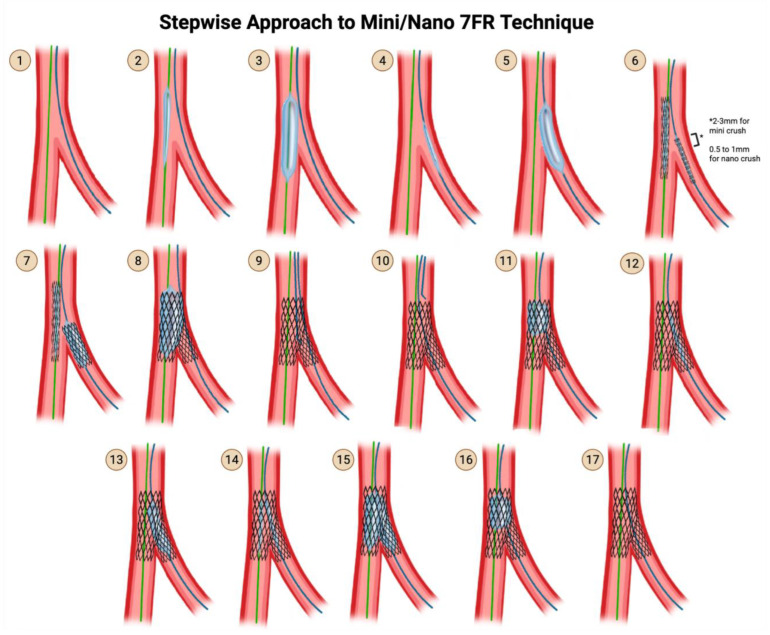
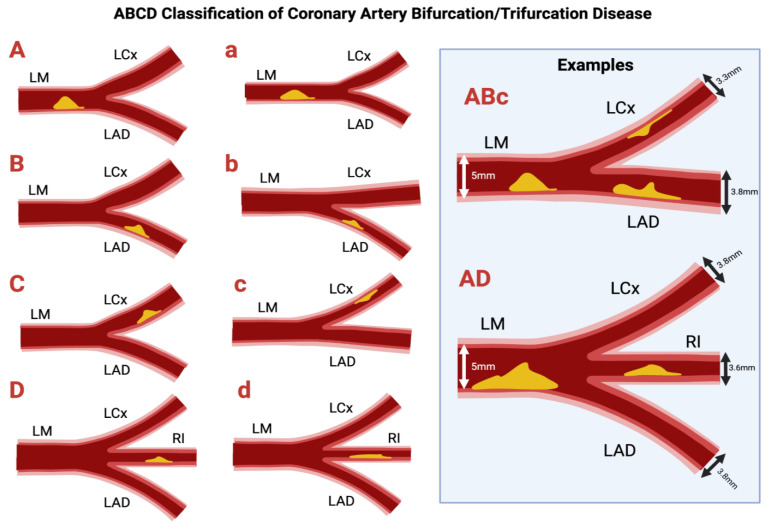
Percutaneous coronary intervention (PCI) of bifurcation lesions remain one of the most technically challenging areas in interventional cardiology. Careful planning and execution are needed to preserve main vessel and side branch patency, with evolving evidence guiding the choice between provisional and two-stent strategies, and between individual techniques. This narrative review, which represents the first installment of a two-part series, synthesizes current knowledge on bifurcation PCI, detailing the anatomical classifications, lesion assessment tools, procedural planning, and execution of techniques including T and Protrusion (TAP), double-kissing (DK) crush, mini-crush, culotte, V-stent, and emerging modifications. We contextualize the choice of strategy within lesion complexity, procedural goals, and patient-specific considerations. This review is intended as a visual, practical, technique-focused reference for interventionalists and interventional trainees involved in the management of bifurcation lesions.
Keywords: bifurcation lesions; bifurcation stenting; coronary artery disease; primary coronary intervention.
Conflict of interest statement
Nanna reports current research support from the American College of Cardiology Foundation, the Patient-Centered Outcomes Research Institute (PCORI), the Yale Claude D. Pepper Older Americans Independence Center (P30AG021342), and the National Institute on Aging (K76AG088428). Nanna also reports being a consultant for Novo Nordisk, Merck, and HeartFlow, Inc. All other authors report no disclosures relevant to the present work.
Figures













References
-
- Burzotta F., Lassen J.F., Lefèvre T., Banning A.P., Chatzizisis Y.S., Johnson T.W., Ferenc M., Rathore S., Albiero R., Pan M., et al. Percutaneous Coronary Intervention for Bifurcation Coronary Lesions: The 15th Consensus Document from the European Bifurcation Club. EuroIntervention. 2021;16:1307–1317. doi: 10.4244/EIJ-D-20-00169. - DOI - PMC - PubMed
-
- Iakovou I., Schmidt T., Bonizzoni E., Ge L., Sangiorgi G.M., Stankovic G., Airoldi F., Chieffo A., Montorfano M., Carlino M., et al. Incidence, Predictors, and Outcome of Thrombosis after Successful Implantation of Drug-Eluting Stents. JAMA. 2005;293:2126–2130. doi: 10.1001/jama.293.17.2126. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
