

A core outcome set for locoregional treatment reporting in neoadjuvant systemic breast cancer treatment trials
- PMID: 41152314
- PMCID: PMC12568921
- DOI: 10.1038/s41523-025-00824-w
A core outcome set for locoregional treatment reporting in neoadjuvant systemic breast cancer treatment trials
Abstract
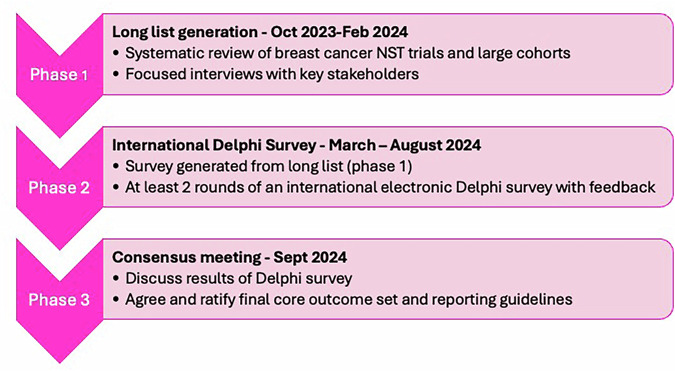
Accurate information about locoregional breast cancer treatments following neoadjuvant systemic therapy (NST) is essential for meaningful interpretation of oncological outcomes but reporting is currently poor. We developed a core outcome set (COS) to improve the quality and consistency of locoregional outcome reporting in breast cancer NST trials. The COS was developed in three phases according to COS-STAD guidance, with the generation of a list of relevant outcome domains, prioritisation of outcomes through two rounds of an international online multi-stakeholder Delphi survey and a consensus meeting. 159 unique locoregional outcomes were classified into 101 outcome domains for inclusion in the Delphi survey, which was completed by 470 international professionals. The final 15-item COS, which included the pre-NST surgical plan, details of surgery performed following completion of treatment and details of radiation therapy, was agreed at an in-person consensus meeting. Widespread COS implementation will improve the quality and value of future NST trials.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: S.P. reports speaker honoraria from Astra Zeneca and BD.SMcI reports speaker honoraria from MSD, Roche, BD, Astra Zeneca, Veracyte and Exact Sciences; advisory boards for Lilly, Novartis, MSD, Roche and Astra Zeneca; conference travel and support from Roche, Lilly and MSD, and institutional research funding from Novartis. J.D.B. reports speaker honoraria from Astra Zeneca, Lily Oncology and Novartis.HI reports consulting fees from Daiichi Sankyo, Chugai, Astra Zeneca, Lilly, MSD, Pfizer and Gilead; honoraria from Daiichi Sankyo, Chugai, Astra Zeneca, Lilly, MSD, Pfizer, Taiho and Kyowa Kirin, and institutional research funding from Chugai, Daiichi Sankyo and Astra Zeneca. P.D. reports institutional research funding from Cepheid and Roche; consulting fees from Roche, and honoraria from Astra Zeneca and Oncoviews, and conference and travel support from Roche.M. Gnant reports personal fees/travel support from Amgen, AstraZeneca, Bayer, DaiichiSankyo, EliLilly, EPG Health (IQVIA), Menarini-Stemline, MSD, Novartis, PierreFabre, Veracyte. H.-B.L. reports research funding from Devicor Medical Product Inc.; speaker honoraria and/or consulting fees from Alvogen, Boryung, Hologic, Intuitive, Lilly, Need, Novartis, Roche, Takeda, Celltrion Pharm, and Shin Poong Pharm; and being a co-founder and member of the DCGen Co., Ltd board of directors, AR reports consulting fees from Astra Zeneca and royalties from Myriad Genetics.GW reports consulting fees from Astra Zeneca, MSD, Novartis, Daiichi Sankyo and Roche; honoraria from Astra Zeneca, MSD, Novartis, Roche, Pfizer and Daiichi-Sankyo, and institutional research funding from Astra Zeneca/Medimmune, Roche/Genentech, GlaxoSmithKline, Novartis, Pfizer, Roche, MSD, Merck, Bayer, Janssen, Astellas Pharma, Libbs and Takeda.NZ reports consulting fees from Lilly, Eisai, Astra Zeneca, MSD, Novartis and Gilead; honoraria from Roche, Pfizer, Eisai, Amgen, Gilead, Novartis, Lilly and Astra Zeneca, and conference travel and support from Novartis, Astra Zeneca and Lilly. AS reports speaker honoraria from Lilly and Limbic. The remaining authors have no conflicts of interest to declare.
References
-
- Spring, L. M., Bar, Y. & Isakoff, S. J. The evolving role of neoadjuvant therapy for operable breast cancer. J. Natl. Compr. Cancer Netw.20, 723–734 (2022). - PubMed
-
- Mamounas, E. et al. Abstract GS02-07: loco-regional irradiation in patients with biopsy-proven axillary node involvement at presentation who become pathologically node-negative after neoadjuvant chemotherapy: primary outcomes of NRG Oncology/NSABP B-51/RTOG 1304. Cancer Res.84, GS02-07–GS02-07 (2024).
-
- von Minckwitz, G. et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N. Engl. J. Med.380, 617–628 (2018). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
