

The international, prospective CytOSorbⓇ treatMent Of critically ill patientS (COSMOS) registry: Interim results from the first 150 patients
- PMID: 41180104
- PMCID: PMC12572895
- DOI: 10.1016/j.jointm.2025.05.001
The international, prospective CytOSorbⓇ treatMent Of critically ill patientS (COSMOS) registry: Interim results from the first 150 patients
Abstract
Background: The CytOSorbⓇ treatMent Of critically ill patientS (COSMOS) registry is an observational, prospective, multicenter, international real-world data collection platform executed in countries where the CytoSorbⓇ (CS) 300 mL device is approved and routinely used in everyday clinical practice. This study aims to investigate utilization patterns of the hemoadsorption device and associated outcomes in critical care.
Methods: Since July 2022, patients who were treated with CS as part of their intensive care treatment were enrolled from 16 sites in Germany, Italy, and Spain in the registry. After informed consent, real-world clinical data are systematically collected at multiple intervals, including 24 h before CS start, during CS treatment, and 24 h post-CS treatment, as well as at discharge from intensive care unit (ICU) and hospital discharge, and final follow-up on day 90. Vital status was assessed as ICU survival, 30-day survival, overall hospital survival, and 90-day survival. We compared details on the type of extracorporeal circuit used, device flow rate, anticoagulation regimen, vasopressor requirements, fluid balance, ratio of partial pressure of oxygen in arterial blood to the fraction of inspiratory oxygen concentration (P/F ratio), myoglobin in the rhabdomyolysis cohort and bilirubin in the liver failure cohort before and after CS treatment. Safety of the device was assessed by investigator-reported device-related adverse effects. Data were presented as either mean ± standard deviation or as median with interquartile range (IQR).
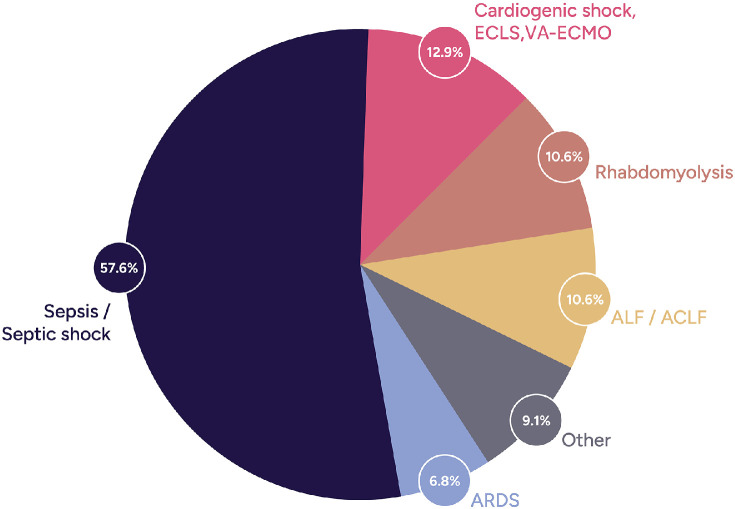
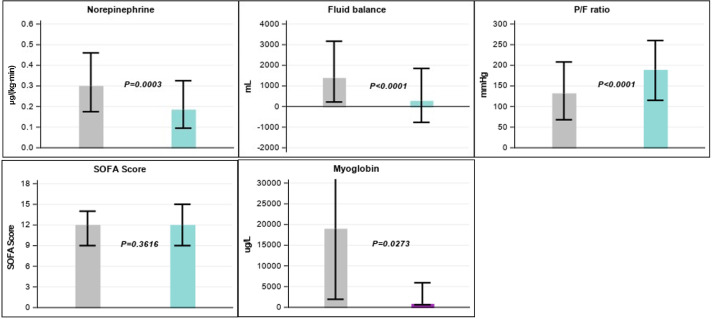
Results: A total of 150 patients were enrolled, 23 patients did not have any data entry by the time of the data readout for this interim analysis conducted and therefore had to be excluded from the analysis (33 % female, mean age [59±17] years). CS indications included septic shock (57.6 %), cardiogenic shock (12.9 %), and rhabdomyolysis (10.6 %). CS was mainly integrated with renal replacement therapy (82.8 %). Median Acute Physiology and Chronic Health Evaluation II score was 23 (IQR: 17-29), Sequential Organ Failure Assessment score 12 (IQR: 9-15), and ICU stay 20 (IQR: 11-33) days. Median interleukin-6 decreased significantly from 862.4 (IQR: 142-97,457) pg/mL in the 24 h before CS treatment to 202.8 (IQR: 42-3247) pg/mL in the 24 h post-CS treatment (P <0.0001). Post-CS, lactate and creatinine levels significantly decreased, fluid balance improved from 1386 (IQR: 220-3168) mL to 275 (IQR: -768-1846) mL (P <0.0001) and median P/F ratio increased from 132 (IQR: 68-208) mmHg to 189 (IQR: 115-260) mmHg (P <0.0001). Norepinephrine requirements reduced from 0.30 (IQR: 0.18-0.46) µg/(kg·min) to 0.19 (IQR: 0.10-0.33) µg/(kg·min) (P=0.0003). In rhabdomyolysis patients, myoglobin decreased from 18,976 (IQR: 1934-34,275) to 835 (IQR: 623-5925) µg/L (P=0.0273). Observed ICU mortality was 35 %, lower than predicted by baseline scores.
Conclusions: The COSMOS registry highlights CS-associated improvements in lactate, creatinine, norepinephrine needs, fluid balance, and oxygenation. Mortality was favorable compared with risk-based predictions.Trial registration Clinicaltrials.gov Identifier: NCT05146336.
Keywords: Adsorption; Blood purification; Cytosorb; Hemoadsorption; Hemoperfusion; Hyperinflammation.
© 2025 The Authors.
Figures
References
-
- Ronco C., Bagshaw S.M., Bellomo R., Clark W.R., Husain-Syed F., Kellum J.A., et al. Extracorporeal blood purification and organ support in the critically ill patient during COVID-19 pandemic: expert review and recommendation. Blood Purif. 2021;50(1):17–27. doi: 10.1159/000508125. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
