Brain dynamics reflecting an intra-network brain state is associated with increased posttraumatic stress symptoms in the early aftermath of trauma
- PMID: 41181354
- PMCID: PMC12574611
- DOI: 10.1038/s44220-024-00377-0
Brain dynamics reflecting an intra-network brain state is associated with increased posttraumatic stress symptoms in the early aftermath of trauma
Abstract
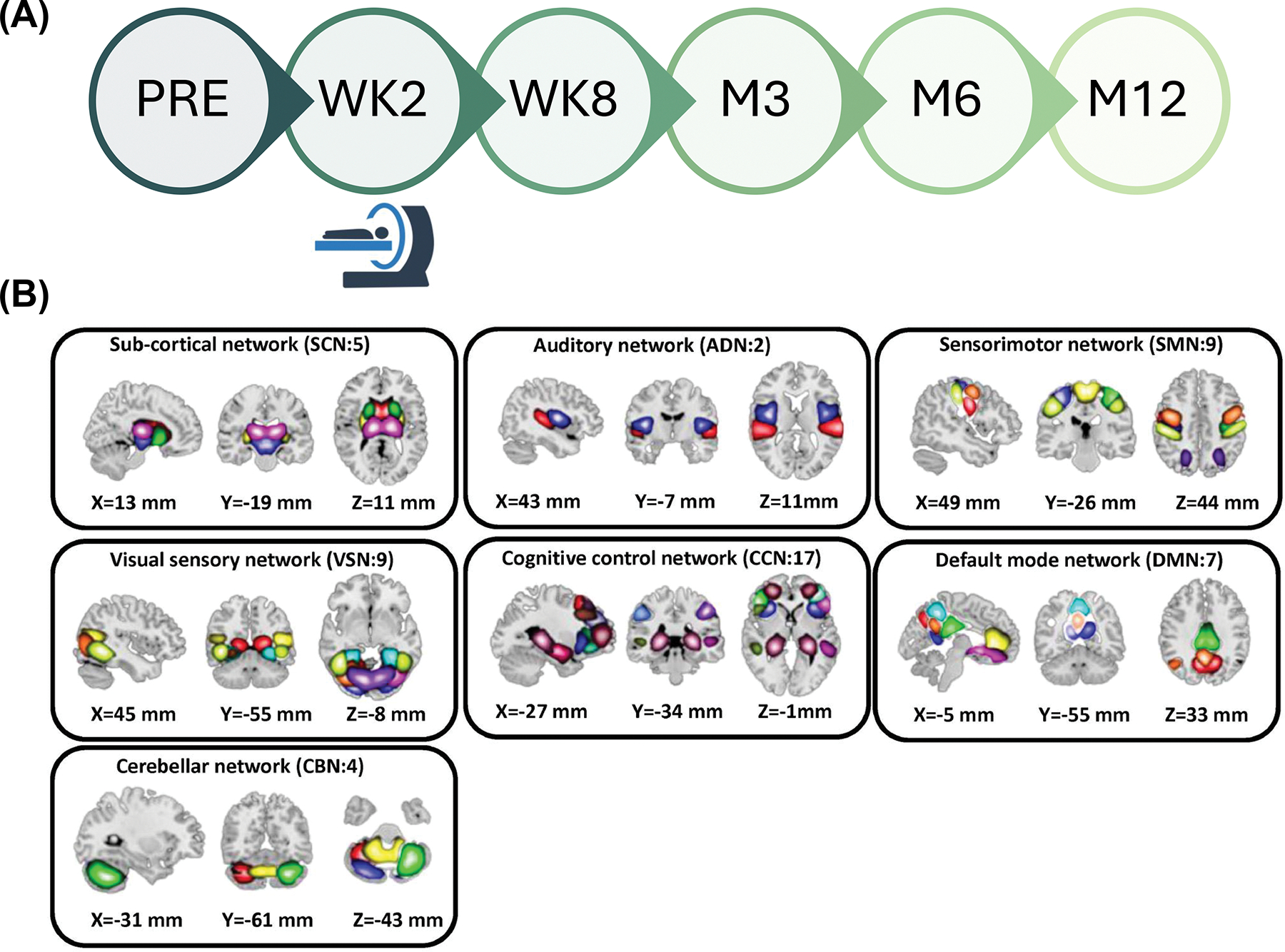
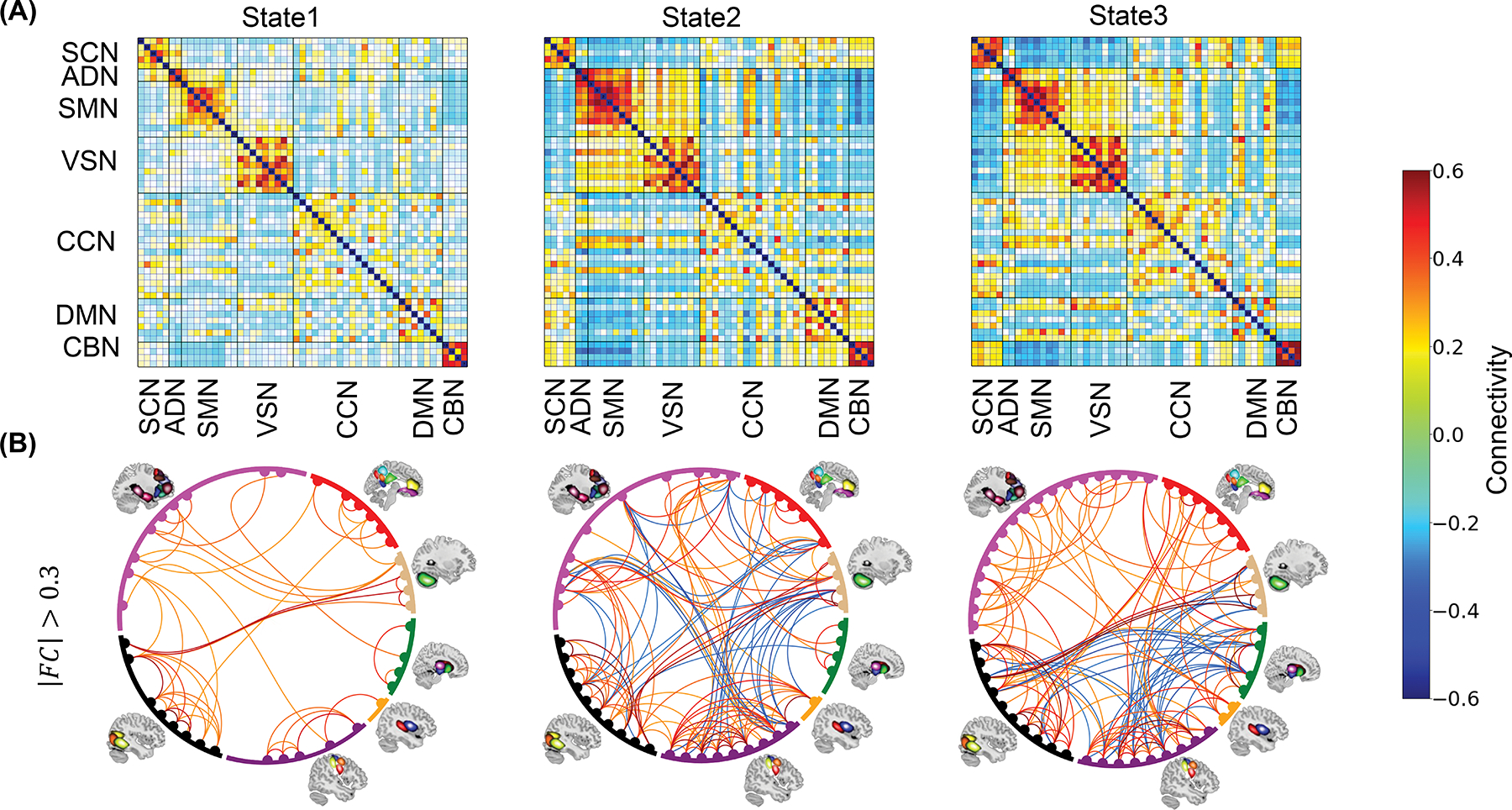
Post-traumatic stress (PTS) encompasses a range of psychological responses following trauma, which may lead to more severe outcomes such as post-traumatic stress disorder (PTSD). Identifying early neuroimaging biomarkers that link brain function to PTS outcomes is critical for understanding PTSD risk. This longitudinal study examines the association between brain dynamic functional network connectivity (dFNC) and current/future PTS symptom severity, and the impact of sex on this relationship. By analyzing 275 participants' dFNC data obtained ~2 weeks after trauma exposure, we noted that brain dynamics of an inter-network brain state link negatively with current (r=-0.197, p corrected = 0.0079) and future (r=-0.176, p corrected = 0.0176) PTS symptom severity. Also, dynamics of an intra-network brain state correlated with future symptom intensity (r = 0.205, p corrected = 0.0079). We additionally observed that the association between the network dynamics of the inter-network and intra-network brain state with symptom severity is more pronounced in female group. Our findings highlight a potential link between brain network dynamics in the aftermath of trauma with current and future PTSD outcomes, with a stronger effect in female group, underscoring the importance of sex differences.
Conflict of interest statement
Competing Interests Statement Dr. Sendi has served as a consulatant for Niji Corp for unrelated work. Dr. Daskalakis is on the scientific advisory board for Sentio Solutions, Inc. and Circular Genomics, Inc. Over the past 3 years, Dr. Pizzagalli has received consulting fees from Boehringer Ingelheim, Compass Pathways, Engrail Therapeutics, Neumora Therapeutics (former BlackThorn Therapeutics), Neurocrine Biosciences, Neuroscience Software, Otsuka Pharmaceuticals, Sage Therapeutics, and Takeda Pharmaceuticals; honoraria from the Psychonomic Society and the American Psychological Association (for editorial work) and Alkermes, and research funding from the Bird Foundation, Brain and Behavior Research Foundation, DARPA, Millennium Pharmaceuticals, and the National Institute of Mental Health. In addition, he has received stock options from Compass Pathways, Engrail Therapeutics, Neumora Therapeutics (former BlackThorn Therapeutics), and Neuroscience Software. Dr. Neylan has received research support from NIH, VA, and Rainwater Charitable Foundation, and consulting income from Jazz Pharmaceuticals. In the last three years Dr Clifford has received research funding from the NSF, NIH and LifeBell AI, and unrestricted donations from AliveCor Inc, Amazon Research, the Center for Discovery, the Gates Foundation, Google, the Gordon and Betty Moore Foundation, MathWorks, Microsoft Research, Nextsense Inc, One Mind Foundation, and the Rett Research Foundation. Dr Clifford has financial interest in AliveCor Inc and Nextsense Inc. He also is the CTO of MindChild Medical with significant stock. These relationships are unconnected to the current work. Dr. Germine is on the board of the Many Brains Project. Her family also has equity in Intelerad Medical Systems, Inc. Dr. Rauch reported serving as secretary of the Society of Biological Psychiatry; serving as a board member of Community Psychiatry and Mindpath Health; serving as a board member of National Association of Behavioral Healthcare; serving as secretary and a board member for the Anxiety and Depression Association of America; serving as a board member of the National Network of Depression Centers; receiving royalties from Oxford University Press, American Psychiatric Publishing Inc, and Springer Publishing; and receiving personal fees from the Society of Biological Psychiatry, Community Psychiatry and Mindpath Health, and National Association of Behavioral Healthcare outside the submitted work. Dr. Jones has no competing interests related to this work, though he has been an investigator on studies funded by AstraZeneca, Vapotherm, Abbott, and Ophirex. Dr. Harte has no competing interest related to this work, though in the last three years he has received research funding from Aptinyx and Arbor Medical Innovations, and consulting payments from Aptinyx. In the past 3 years, Dr. Kessler was a consultant for Cambridge Health Alliance, Canandaigua VA Medical Center, Holmusk, Partners Healthcare, Inc., RallyPoint Networks, Inc., and Sage Therapeutics. He has stock options in Cerebral Inc., Mirah, PYM, and Roga Sciences. Dr. Koenen’s research has been supported by the Robert Wood Johnson Foundation, the Kaiser Family Foundation, the Harvard Center on the Developing Child, Stanley Center for Psychiatric Research at the Broad Institute of MIT and Harvard, the National Institutes of Health, One Mind, the Anonymous Foundation, and Cohen Veterans Bioscience. She has been a paid consultant for Baker Hostetler, Discovery Vitality, and the Department of Justice. She has been a paid external reviewer for the Chan Zuckerberg Foundation, the University of Cape Town, and Capita Ireland. She has had paid speaking engagements in the last three years with the American Psychological Association, European Central Bank. Sigmund Freud University – Milan, Cambridge Health Alliance, and Coverys. She receives royalties from Guilford Press and Oxford University Press. Dr. McLean has served as a consultant for Walter Reed Army Institute for Research, Arbor Medical Innovations, and BioXcel Therapeutics, Inc. Dr. Ressler has performed scientific consultation for Bioxcel, Bionomics, Acer, and Jazz Pharma; serves on Scientific Advisory Boards for Sage, Boehringer Ingelheim, Senseye, and the Brain Research Foundation, and he has received sponsored research support from Alto Neuroscience. The remaining authors declare no competing interests.
Figures