

Effect of day 3 cell number on the pregnancy and neonatal outcomes of vitrified-warmed single blastocyst transfer
- PMID: 41194271
- PMCID: PMC12587729
- DOI: 10.1186/s40001-025-03343-3
Effect of day 3 cell number on the pregnancy and neonatal outcomes of vitrified-warmed single blastocyst transfer
Abstract
Background: The aim of this retrospective cohort study was to evaluate the effect of day 3 embryo cell number on the clinical pregnancy and neonatal outcomes of single blastocyst transfer in frozen embryo transfer (FET) cycles.
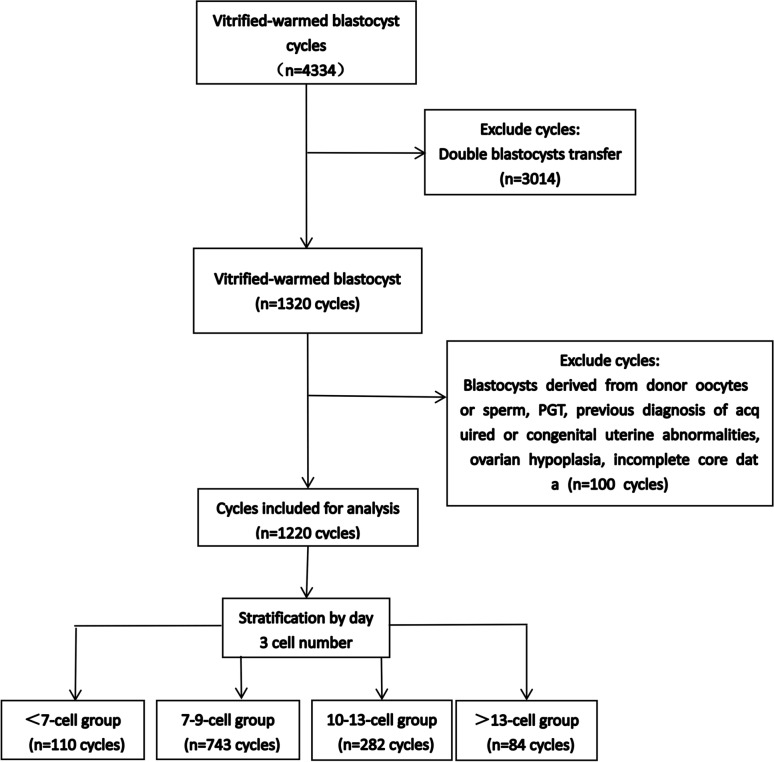
Methods: The study included 1220 single blastocyst transfer from FET cycles conducted between January 2017 and April 2024. Patients were categorized into four groups based on day 3 embryo cell number : 110 cycles in the < 7-cell group, 743 cycles in the 7-9-cell group, 282 cycles in the 10-13-cell group, and 84 cycles in the > 13-cell group. The study compared the clinical pregnancy outcomes and neonatal outcomes among the four groups.
Results: When the maternal age was < 35 years or high-quality blastocysts were transferred, the clinical pregnancy rate (CPR) of the < 7-cell group was significantly lower than those of other three groups (all P < 0.008). Similarly, when high-quality blastocysts were transferred, the live birth rates (LBRs) of the 7-9-cell group and > 13-cell group were significantly higher than those of the < 7-cell group (all P < 0.008). In women aged < 35 years with high-quality blastocyst transfers, after adjusting for confounders, 7-9 and 10-13 groups were with significantly higher CPR (aOR 2.66, 95% CI 1.44-4.91; aOR 2.15, 95%CI 1.10-4.18 and LBR (aOR 2.50, 95%CI 1.32-4.73, aOR 1.74, 95% CI 0.88-3.46).
Conclusion: In FET cycles, a low day 3 cell number (< 7-cell) on day 3 was related to decreased CPR and LBR after blastocyst transfer, whereas a number > 9 was comparable to that of 7-9 cells.
Keywords: Blastocyst; Cell number; Clinical pregnancy; Frozen embryo transfer; Live birth; Neonatal.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study followed the Declaration of Helsinki and was performed in accordance with the relevant local guidelines and regulations. The study was approved by the research ethics board at Xingtai Meihe Reproductive and Genetic Hospital (approval number: 2023-15). The requirement for informed consent was waived owing to the retrospective nature of the study, and data from all patients were used anonymously. The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
