

Treatment patterns of empirical antibiotic therapies for critically ill patients with sepsis: a cross-sectional study in Vietnam
- PMID: 41214528
- PMCID: PMC12604204
- DOI: 10.1186/s12879-025-11992-2
Treatment patterns of empirical antibiotic therapies for critically ill patients with sepsis: a cross-sectional study in Vietnam
Abstract
Background: A systematic description of patterns of empirical antibiotic therapies (EAT) and the factors driving these in critically ill patients with sepsis is lacking in resource-limited settings. We aimed to address this knowledge gap by exploring the EAT patterns and risk factors for deviations from the guidelines in EAT in a Vietnamese hospital.
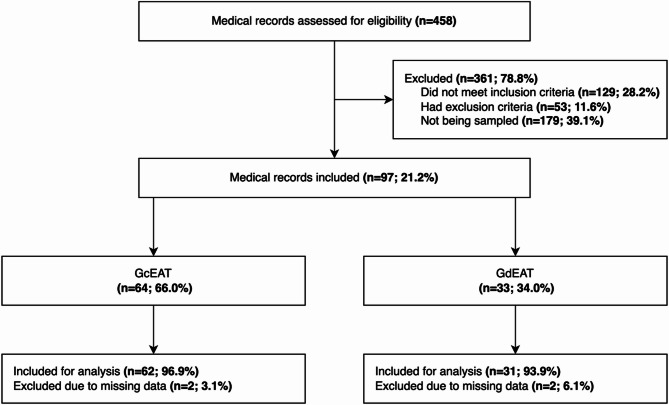
Methods: We conducted a simple random-sampling cross-sectional study at the intensive care unit (ICU) using medical records of critically ill patients with sepsis. The outcomes were guideline-compliant and guideline-deviant EAT (GcEAT and GdEAT). GcEAT was full compliance (choice and dosage) with local protocol for sepsis management, while GdEAT was any treatment that was not GcEAT. We used descriptive statistics to present data. Risk factors for GdEAT were reported with adjusted odds ratio, 95% confidence interval (OR and 95% CI; using multivariable logistic regression) and E-value (for factors with significant associations).
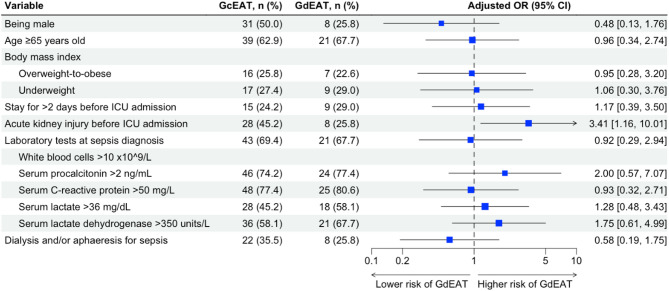
Results: Among 93 medical records included for analysis (median age of 68, 41.9% being male, 24.7% being overweight-to-obese). Initiation through the concurrent administration of three antibiotic agents was reported in 37.6% of all cases (96.8% with pseudomonal coverage, 91.4% with anaerobic coverage, 34.4% with MRSA coverage, 49.5% with enterococcal coverage). GcEAT was detected in 62 records (66.7%, 95% CI 56.6% to 75.4%), while GdEAT was in 31 records (33.3%, 95% CI 24.6% to 43.4%). The specific patterns in the GdEAT group were: (1) broader/narrower antibacterial coverage (87.1%) and overlapping targets (12.9%) (for choice of EAT), (2) higher/lower doses (45.2%), longer/shorter dosing intervals (38.7%), and without therapeutic drug monitoring (16.1%) (for dosage of EAT). Acute kidney injury before ICU admission was identified as a potential risk factor for GdEAT (adjusted OR 3.41, 95% CI 1.16 to 10.01; E-value 3.10, lower bound of CI 1.37), which was mainly driven by deviations in the dosage of EAT (adjusted OR 3.45, 95% 1.18 to 10.08; E-value 3.12, lower bound of CI 1.39).
Conclusion: GdEAT was moderately prevalent in sepsis management of critically ill patients at a Vietnamese healthcare setting, primarily due to deviations in choice and dosage of the EAT. Further research and updated guidelines should address the optimal EAT in patients with acute kidney injury to avoid unstandardised deviations and noncompliances with antimicrobial protocols.
Clinical trial number: Not applicable.
Keywords: Critical illness; Empirical antibiotic; Perioperative care; Risk factors; Sepsis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Institutional Review Board of the University of Medicine and Pharmacy at Ho Chi Minh City, under approval number 1018/HDDD-DHYD. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Garnacho-Montero J, Garcia-Garmendia JL, Barrero-Almodovar A, Jimenez-Jimenez FJ, Perez-Paredes C, Ortiz-Leyba C. Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit Care Med. 2003;31(12):2742–51. 10.1097/01.Ccm.0000098031.24329.10. - PubMed
-
- Lindberg O, De Geer L, Chew MS. Nonadherence to antibiotic guidelines in patients admitted to ICU with sepsis is associated with increased mortality: A registry-based, retrospective cohort study. Eur J Anaesthesiol. 2020;37(2):113–20. 10.1097/eja.0000000000001140. - PubMed
-
- Vazquez-Guillamet C, Scolari M, Zilberberg MD, Shorr AF, Micek ST, Kollef M. Using the number needed to treat to assess appropriate antimicrobial therapy as a determinant of outcome in severe sepsis and septic shock. Crit Care Med. 2014;42(11):2342–9. 10.1097/ccm.0000000000000516. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
