

Ketogenic diet for status epilepticus in adult intensive care unit patients: a standard operating procedure
- PMID: 41225685
- PMCID: PMC12613490
- DOI: 10.1186/s42466-025-00431-x
Ketogenic diet for status epilepticus in adult intensive care unit patients: a standard operating procedure
Abstract
Introduction: Refractory and super-refractory status epilepticus (RSE and SRSE) are life-threatening neurological emergencies with significant morbidity and mortality. When conventional treatment strategies, including antiseizure medications (ASM) and anesthetic agents, fail, alternative metabolic approaches, such as the ketogenic diet (KD), have been considered. KD is a high-fat, low-carbohydrate, and adequate-protein diet that induces ketosis, exerting anticonvulsant effects. Different types of KD are available, including the classical KD and the modified Atkins diet (MAD). Most published evidence in RSE and SRSE stems from classical KD protocols with high fat-to-carbohydrate/protein ratios (e.g., 4:1), whereas evidence for MAD in this setting is limited, and outcome equivalence across KD types remains unclear. While emerging evidence suggests efficacy in RSE and SRSE, clinical application in adult intensive care unit (ICU) settings remains inconsistent. This standard operating procedure (SOP), developed collaboratively by neurologists, intensivists, anesthesiologists, and clinical nutrition experts, provides a structured framework for classical KD implementation in adult ICU patients with RSE and SRSE, covering indications, contraindications, initiation, monitoring, and safety considerations.
Definition: KD is a metabolic therapy that induces ketosis, providing an alternative energy source for the brain while modulating neurotransmitter activity and neuronal excitability.
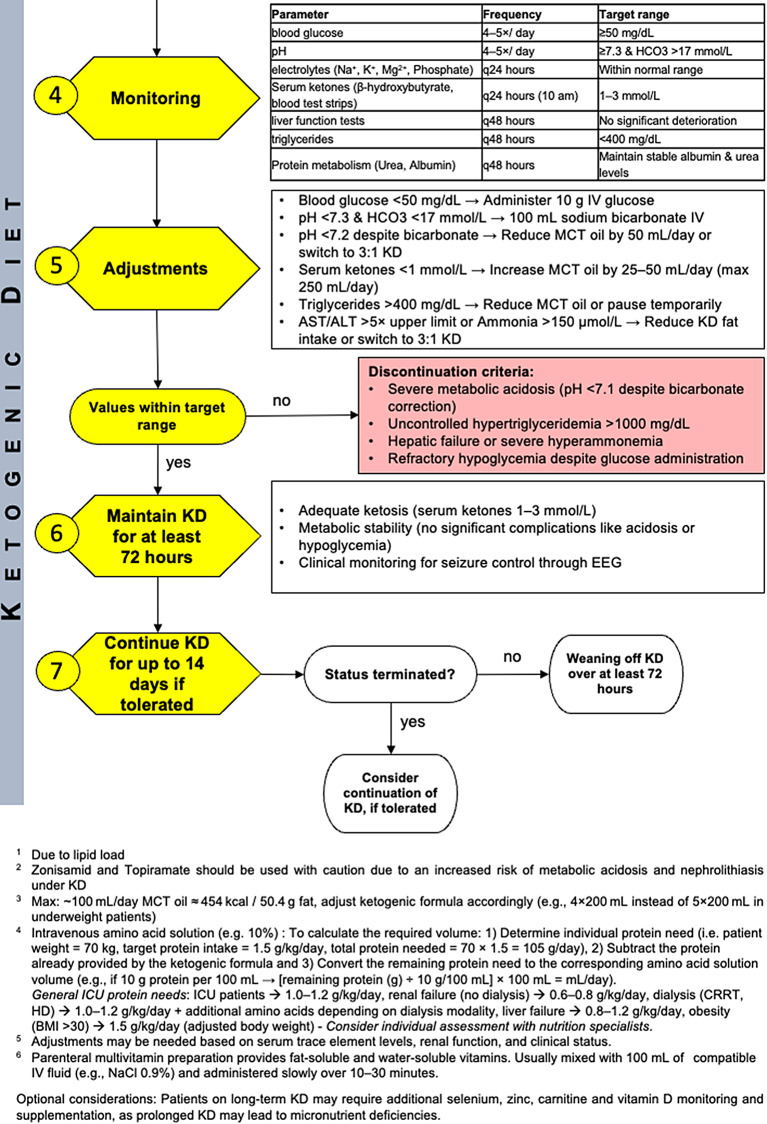
First steps: KD should be considered in RSE persisting for > 72 h despite adequate antiseizure treatment or in SRSE early after ICU admission, preferably within 24 h. Before initiation, metabolic screening is required, including tests on liver and renal function, lipid profile, electrolyte balance, and glucose metabolism. Absolute contraindications, such as severe hepatic dysfunction, ileus, or severe hypertriglyceridemia, must be ruled out. Continuous EEG monitoring should be considered. The diet is typically initiated using a classical KD protocol with a 4:1 lipid-to-non-lipid ratio formula and stepwise fat increase, supplemented with medium-chain triglyceride (MCT) oil to enhance ketosis. Essential micronutrients, including carnitine, vitamins, and trace elements, should be supplemented routinely based on clinical indication to prevent deficiencies.
Comments: KD initiation follows a stepwise protocol with enteral formulations. Strict biochemical monitoring is essential to ensure metabolic stability, focusing on glucose, ketone levels, lipid profiles, liver function, and acid-base balance. Adverse effects, including metabolic acidosis, hypoglycemia, and hyperlipidemia, require timely adjustments. Involvement of an experienced dietician for nutritional support, trained nursing staff, as well as close interdisciplinary coordination are critical for successful initiation and maintenance of KD and for minimizing complications, particularly in centers with limited KD experience due to lack of familiarity with ketosis-impeding factors such as carbohydrate-containing medications. The suggested flowchart provides a structured approach for decision-making, highlighting indications, monitoring strategies, and emergency discontinuation criteria.
Conclusion: This SOP provides a standardized, interdisciplinary protocol for classical KD implementation in adult ICU patients with RSE and SRSE. Developed collaboratively it integrates current literature and institutional experience. Despite heterogeneous study results, we advocate for early KD initiation in all SRSE patients without contraindications, given its safety, reversibility, and rapid implementability. By enhancing reproducibility and clinical feasibility, this SOP offers a practical and transferable tool for neurocritical care. We encourage other centers to adapt and apply this approach to further validate its utility.
Keywords: Ketogenic diet; Refractory status epilepticus; Standard operational procedure; Supra-refractory status epilepticus.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: KF received grants from the university of Tübingen (AKF and Sigrid-Örgel Stiftung) and speakers’ honoraria/consulting fees from AstraZeneca and BMS/Pfizer, all not related to this work. DS, MA, SK, and CS report no conflict of interest. FB received speakers’ honoraria/consulting fees from Nutricia, Jazz Pharmaceuticals, UCB, Angelini Pharma, all not related to this work. JB received speaker honoraria and travel support from Boehringer, Medtronic, Neuroptics, TelaDoc; Award participation in PCORI Award for SETPOINT2 all not related to this work. AM received grants from the university of Tübingen (AKF) and speakers’ honoraria/consulting fees from AMGEN, all not related to this work. Consent to publish: We hereby confirm that all authors have read the submitted manuscript in its entirety and consent to its publication.
Figures

References
-
- Trinka, E., et al. (2015). A definition and classification of status epilepticus–Report of the ILAE task force on classification of status epilepticus. Epilepsia, 56(10), 1515–1523. - PubMed
-
- Trinka, E., & Leitinger, M. (2022). Management of status epilepticus, refractory status epilepticus, and Super-refractory status epilepticus. Continuum (Minneap Minn), 28(2), 559–602. - PubMed
-
- Kantanen, A. M., et al. (2015). Incidence and mortality of super-refractory status epilepticus in adults. Epilepsy & Behavior, 49, 131–134. - PubMed
-
- Johnson, E. L., & Kaplan, P. W. (2020). Status epilepticus: Definition, Classification, Pathophysiology, and epidemiology. Seminars in Neurology, 40(6), 647–651. - PubMed
-
- Vignatelli, L., et al. (2024). Clinical practice guidelines on the management of status epilepticus in adults: A systematic review. Epilepsia, 65(6), 1512–1530. - PubMed
LinkOut - more resources
Full Text Sources