

Real-world oncologic outcomes of thoracoscopic and open tracheal cancer resection
- PMID: 41229748
- PMCID: PMC12603544
- DOI: 10.21037/jtd-2025-1445
Real-world oncologic outcomes of thoracoscopic and open tracheal cancer resection
Abstract
Background: Minimally invasive video-assisted thoracoscopic surgery (VATS) for tracheal cancer is gaining popularity. However, data are limited to single-center reports and short-term outcomes. In this context, we aim to compare short and long-term oncologic outcomes of VATS versus open tracheal cancer resection at the national level.
Methods: We used a national dataset to isolate primary tracheal cancers diagnosed between 2010-2021. Patients were stratified by operative approach into open and VATS resection groups. Cox analysis was used to estimate proportional effects of covariates in unmatched cohorts. We then used propensity score matching to minimize confounding bias from covariates. Kaplan-Meier survival analyses were used to estimate 5-year survival.
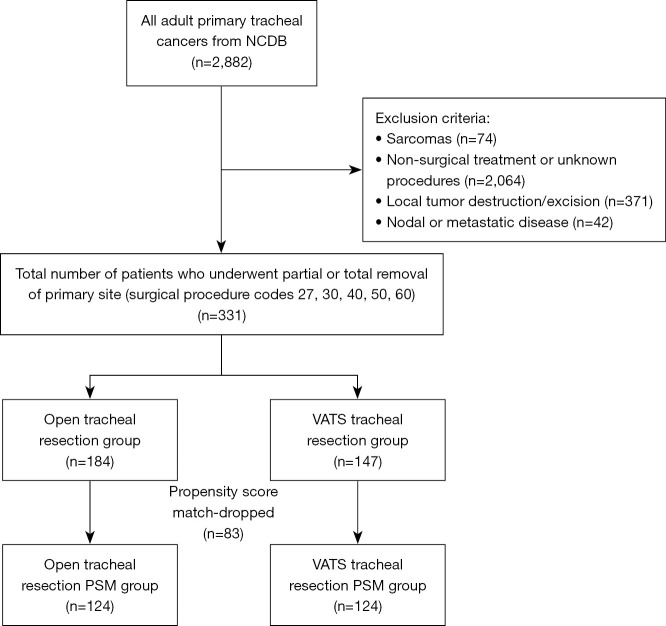
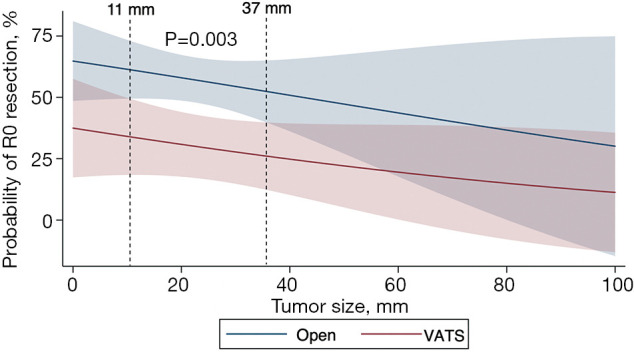
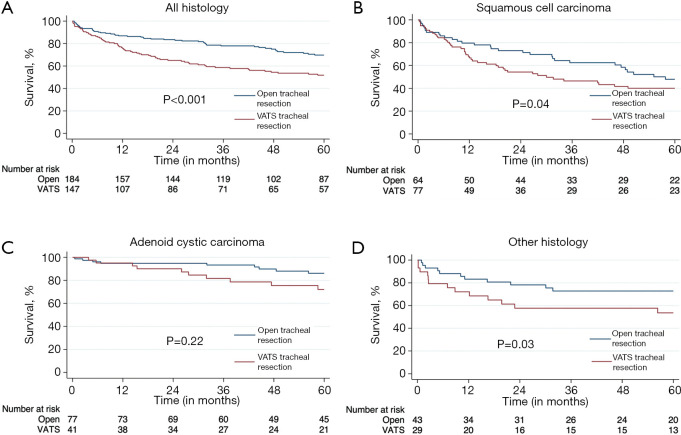
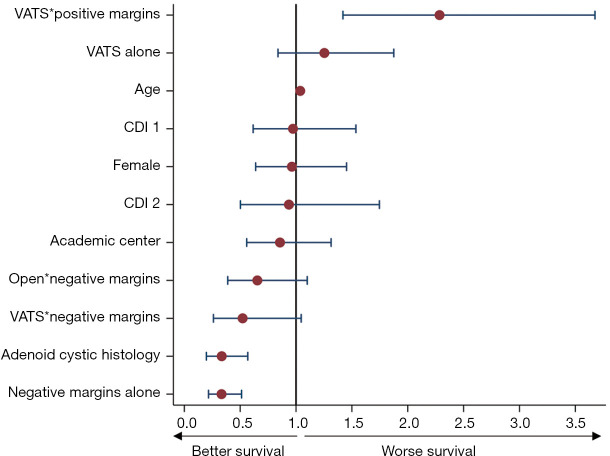
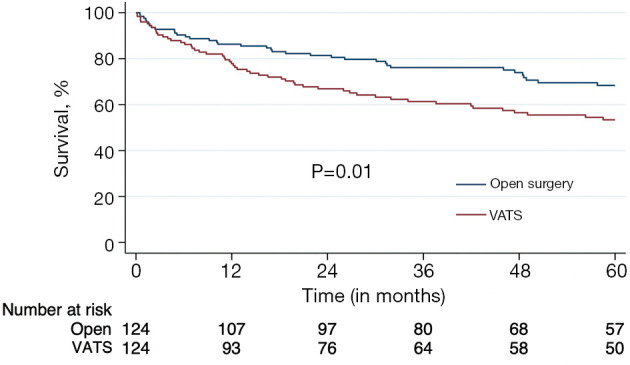
Results: Of 331 patients undergoing tracheal cancer resection, 147 (44.4%) were started VATS with 5 (3.4%) converting to open. Patients undergoing VATS tracheal resection were similar in age (62.4±14.5 vs. 59.9±14.2 years; P=0.12), race (White =81.0% vs. 84.8%; P=0.32) and Charlson-Deyo comorbidity (index =0, 59.2% vs. 68.5%; P=0.19), but were more likely to be male (57.8% vs. 46.2%; P=0.04) and have positive margins (58.1% vs. 41.0%; P=0.006) compared to open resection. Post-operative length of stay was shorter with VATS (median 2.5 vs. 7.0 days; P<0.001), but this came at the expense of higher rates of positive margins [adjusted odds ratio (aOR) =2.15, P=0.02] and worse median survival (74 vs. 106 months; P<0.001), which persisted after matching (79 vs. 100 months; P=0.01).
Conclusions: In this national observational study, we found that the short-term benefits of thoracoscopic tracheal resection come at the expense of increased positive margins and worse survival. Adoption of this approach for tracheal cancer should be met with caution.
Keywords: Tracheal cancer; open surgery; video-assisted thoracoscopic surgery (VATS).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-1445/coif). Z.M.A. serves as an unpaid editorial board member of Journal of Thoracic Disease from December 2023 to November 2025. The other authors have no conflicts of interest to declare.
Figures
References
-
- Shah P, Kela K, Hegde UP. Tracheal cancer epidemiology and survival trends: A SEER database analysis. J Clin Oncol 2024;42:e20078.
LinkOut - more resources
Full Text Sources
Miscellaneous