

Characterization of pleural metastasis in non-small cell carcinomas undergoing intraoperative frozen section examination
- PMID: 41229767
- PMCID: PMC12603490
- DOI: 10.21037/jtd-2025-1511
Characterization of pleural metastasis in non-small cell carcinomas undergoing intraoperative frozen section examination
Abstract
Background: Pleural biopsy via open surgery or video-assisted thoracoscopic surgery is consistently performed in patients with non-small cell lung carcinoma (NSCLC) for diagnostic tumor confirmation, tumor staging, and tumor tissue acquisition. We investigated the clinicopathological characteristics of pleural metastasis in NSCLC, with a specific focus on the comparison between adenocarcinoma (ADC) and squamous cell carcinoma (SqCC). This study aimed to quantify how intraoperative gross finding predicts a positive-for-malignancy (PFM) diagnosis on frozen sections and to delineate histology-specific microscopic features distinguishing ADC from SqCC in PFM cases.
Methods: A retrospective analysis was conducted on 237 pleural biopsies, which underwent intraoperative frozen examination between March 2000 and February 2015. Clinicopathologic parameters, including intraoperative visual inspection and microscopic findings, were assessed in 112 NSCLC patients (75 ADC and 37 SqCC).
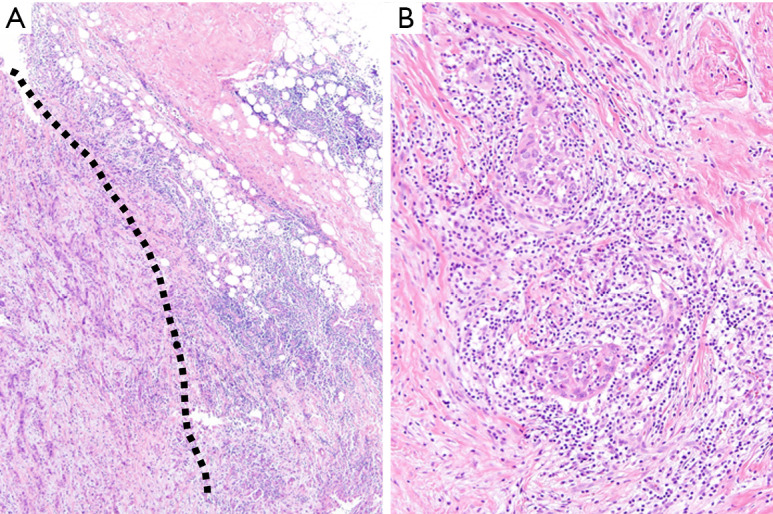
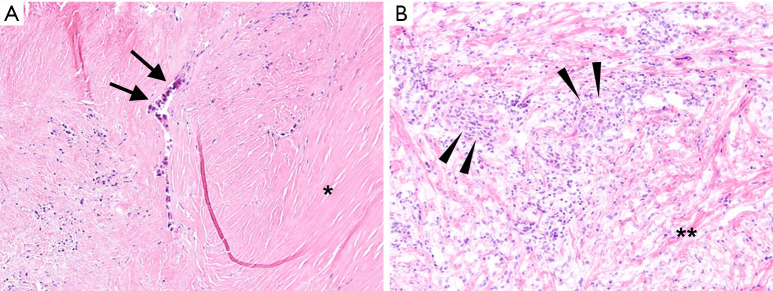
Results: Among 112 NSCLC cases, the presence of pleural nodularity during the operative procedure was identified as an independent predictor for pleural metastasis [odds ratio (OR) 8.33, 95% confidence interval (CI): 3.36-20.65, P<0.001]. Microscopic examination revealed that sclerotic fibrosis was associated with pleural metastasis in ADC (OR 6.56, 95% CI: 1.71-25.26, P=0.006), whereas metastatic SqCC exhibited a higher inflammatory component than ADC (80.0% vs. 30.1%, P<0.001), albeit without significant prediction for pleural metastasis in SqCC.
Conclusions: Pleural nodularity in operative field strongly indicated pleural metastasis in NSCLC. Additionally, ADC and SqCC exhibited distinct microscopic characteristics, with sclerotic fibrosis frequently accompanying pleural metastasis in ADC.
Keywords: Non-small cell lung carcinoma (NSCLC); frozen section; metastasis; pathology; pleura.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-1511/coif). The authors have no conflicts of interest to declare.
Figures

References
-
- SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2025 Jul 2. [cited 2025 Sep 9]. Available from: https://seer.cancer.gov/statistics-network/explorer/. Data source(s): SEER Incidence Data, November 2024 Submission (1975-2022), SEER 21 registries.
LinkOut - more resources
Full Text Sources