

Intrathoracic retention time of pericardial fat pads without pedicle in bronchial stump coverage: insights from a retrospective study
- PMID: 41229868
- PMCID: PMC12603409
- DOI: 10.21037/jtd-2025-896
Intrathoracic retention time of pericardial fat pads without pedicle in bronchial stump coverage: insights from a retrospective study
Abstract
Background: Bronchopleural fistula (BPF) is a severe complication after anatomical pulmonary resection. The incidence is low, but the mortality rate is high. Risk factors include the site of resection (right pneumonectomy or right lower lobectomy, neoadjuvant therapy, and poor nutritional status. While bronchial stump coverage by autologous tissue reduces the risk of BPF, the optimal tissue for coverage remains unclear. The aim of this study was to evaluate the residual rate of free pericardial fat pad (FPFP) remaining in the thoracic cavity and to investigate whether covering bronchial stump with FPFP is effective for preventing BPF.
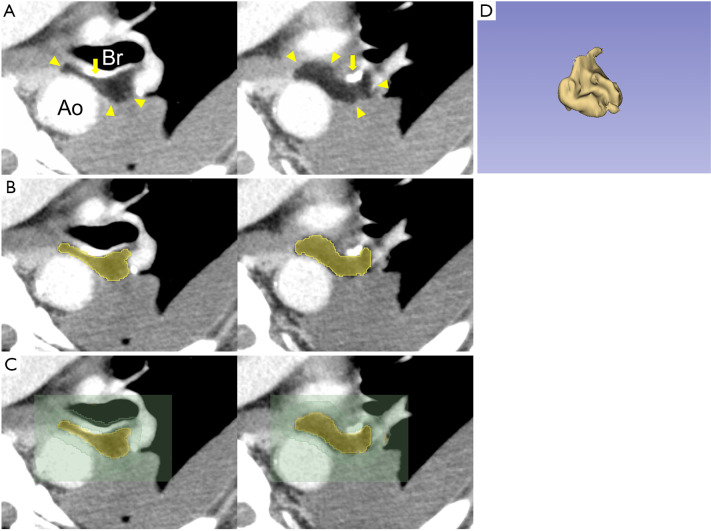
Methods: This retrospective study analyzed the residual rate of FPFP postoperatively and risk factors for BPF. Participants comprised 1,745 patients who underwent radical pulmonary resection. In 45 cases, the residual volume of FPFP was assessed from computed tomography (CT) using the 3D Slicer imaging computing platform.
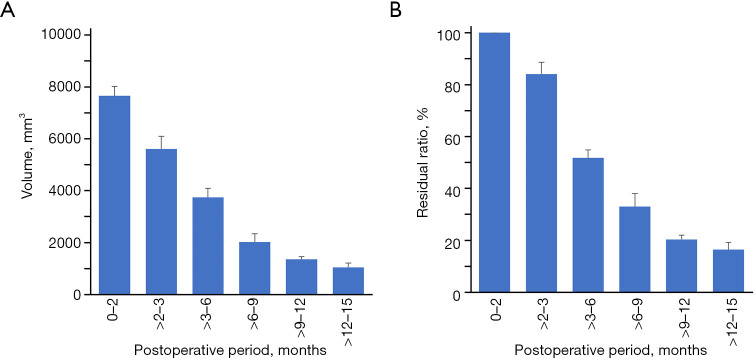
Results: The volume of FPFP was 84% at 3 months postoperatively, and >50% at 6 months postoperatively. The bronchial closure site remained fully covered in all cases at 3-6 months. Multivariate analysis revealed serum albumin level <4.1 g/dL, lower lobectomy, lymph node dissection, and postoperative pneumonia as significant independent risk factors for BPF.
Conclusions: Despite being a minimally invasive method with non-vascularized autologous tissue, FPFP retained more than half its volume for approximately 6 months postoperatively. These findings suggest the possibility that FPFP coverage of the bronchial stump may prevent BPF.
Keywords: Bronchopleural fistula (BPF); anatomical pulmonary resection; free pericardial fat pad (FPFP).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-896/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Jacobsen K. Bronchopleural Fistula after Pulmonary Resection: Risk Factors, Diagnoses and Management. IntechOpen 2022. doi: 10.5772/intechopen.100209 - DOI
LinkOut - more resources
Full Text Sources