

Gastropleurocutaneous fistula secondary to cement prosthesis migration: A rare late complication of chest wall sarcoma reconstruction
- PMID: 41250093
- PMCID: PMC12625230
- DOI: 10.1186/s12893-025-03312-x
Gastropleurocutaneous fistula secondary to cement prosthesis migration: A rare late complication of chest wall sarcoma reconstruction
Abstract
Background: Gastropleurocutaneous fistula (GPCF) is a rare, potentially life-threatening condition defined by an abnormal connection between the stomach and the pleural cavity with an accompanying cutaneous tract. It is distinct from a gastropleural fistula, which lacks an external cutaneous extension. To our knowledge, no prior reports have described GPCF caused by migration and erosion of a cement chest-wall prosthesis.
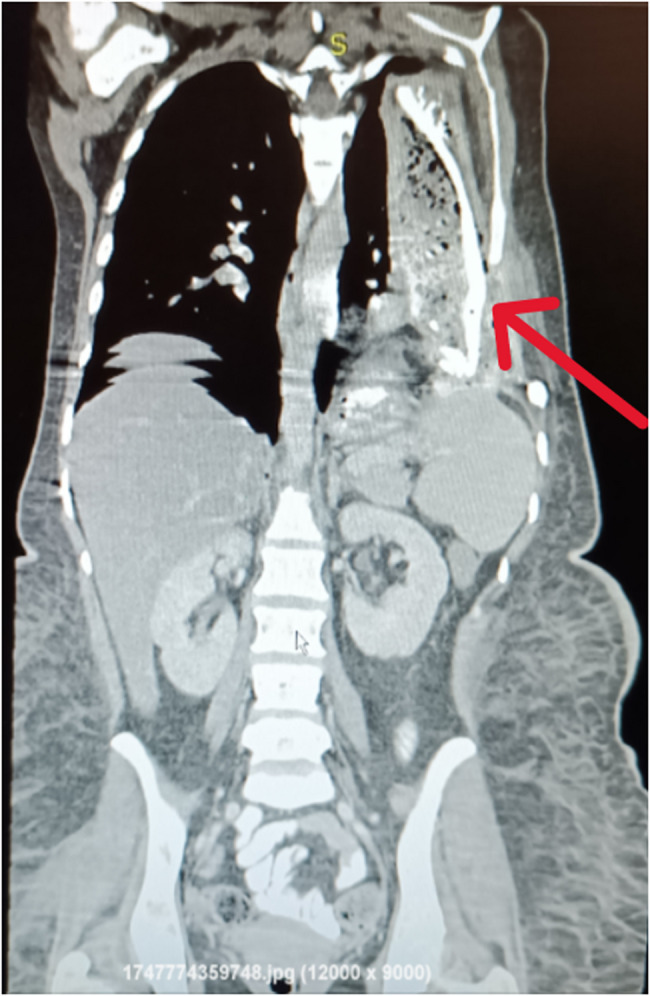
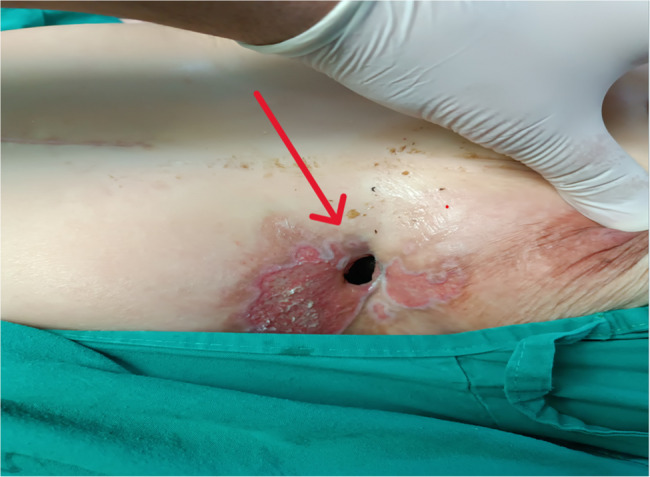
Case presentation: We present the case of a 40-year-old female with a history of anterior chest wall sarcoma resection and cement prosthesis reconstruction performed 23 years earlier. The patient developed a chronic cutaneous discharge beneath the left breast and was ultimately diagnosed with a gastropleurocutaneous fistula. Although she had experienced prior episodes of discharge, this was the first time the condition was confirmed through imaging and intraoperative findings. Imaging revealed a large left thoracoabdominal collection and erosion of the diaphragm by the prosthesis into the gastric fundus. Surgical management included isolation and stapling of the gastric fistula, diaphragmatic repair using polypropylene mesh, and pleural cavity debridement.
Case discussion: The development of gastropleurocutaneous fistula secondary to cement prosthesis migration has not been previously documented. While cement-based prostheses offer structural stability, long-term complications such as erosion into visceral organs may occur, particularly with inadequate fixation or soft tissue coverage. Diagnosis requires a high index of suspicion and a combination of radiological and endoscopic modalities. Surgical repair remains the definitive treatment, often requiring a combined thoracoabdominal approach.
Conclusion: This case highlights a rare but serious late complication of chest wall reconstruction with cement prosthesis. It underscores the need for long-term surveillance in patients with synthetic implants and the importance of individualized surgical planning in managing complex thoracoabdominal fistulas.
Keywords: Case report; Cement prosthesis migration; Chest wall reconstruction; Chest wall sarcoma; Diaphragmatic repair; Gastropleurocutaneous fistula; Polymethylmethacrylate (PMMA); Prosthesis erosion; Surgical complication; Thoracoabdominal fistula.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Institutional review board approval was not required for this de-identified single case report in accordance with the policies of Al-Mouwasat University Hospital, Faculty of Medicine, Damascus University. Consent for publication: Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request. Competing interests: The authors declare no competing interests.
Figures


References
-
- Nguyen D, Dip F, Hendricks L, Lo Menzo E, Szomstein S, Rosenthal R. The surgical management of complex fistulas after sleeve gastrectomy. Obes Surg. 2016;26(2):245–50. 10.1007/s11695-015-1788-2. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
