

This is a preprint.
Fetal monitoring using a wearable ultrasound patch for high-risk pregnancies
- PMID: 41282201
- PMCID: PMC12632705
- DOI: 10.21203/rs.3.rs-7715480/v1
Fetal monitoring using a wearable ultrasound patch for high-risk pregnancies
Abstract
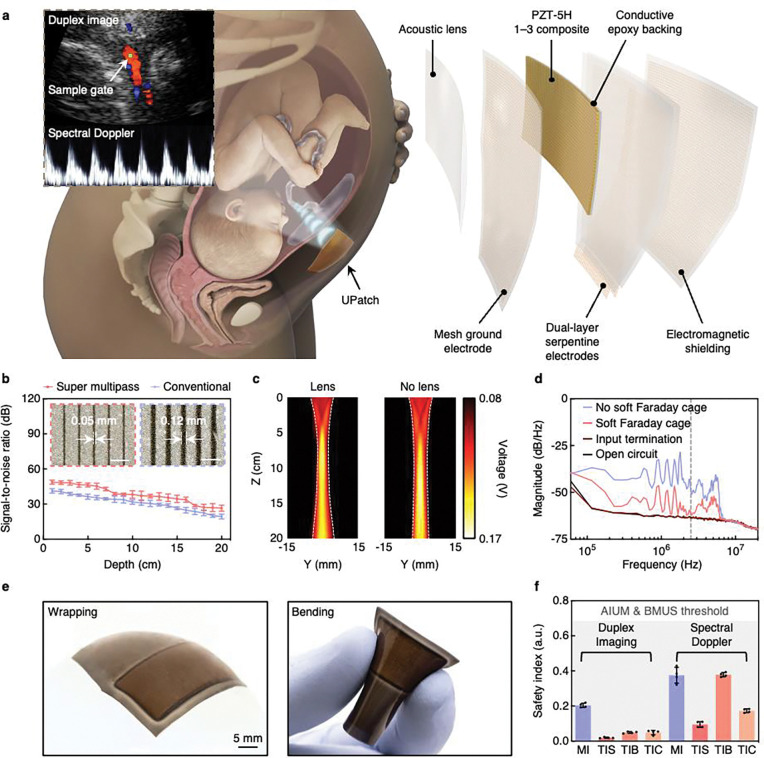
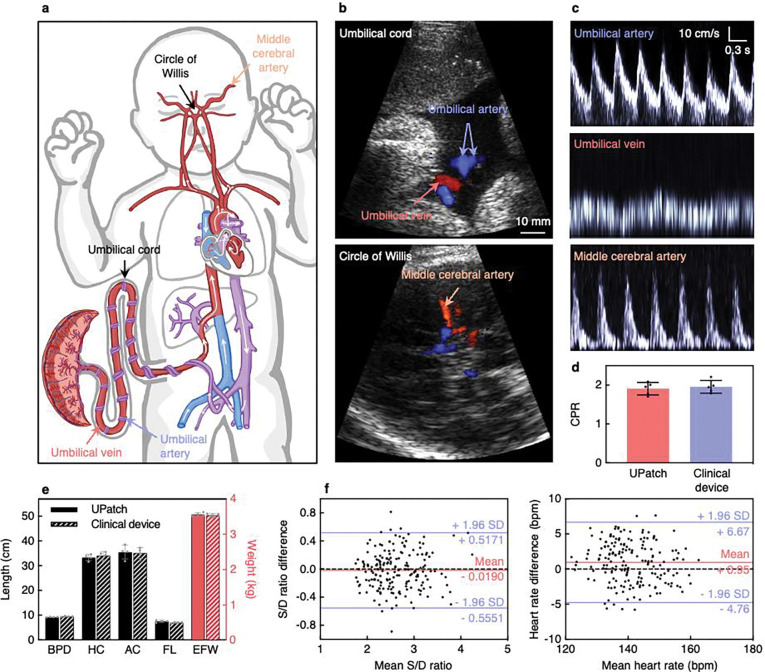
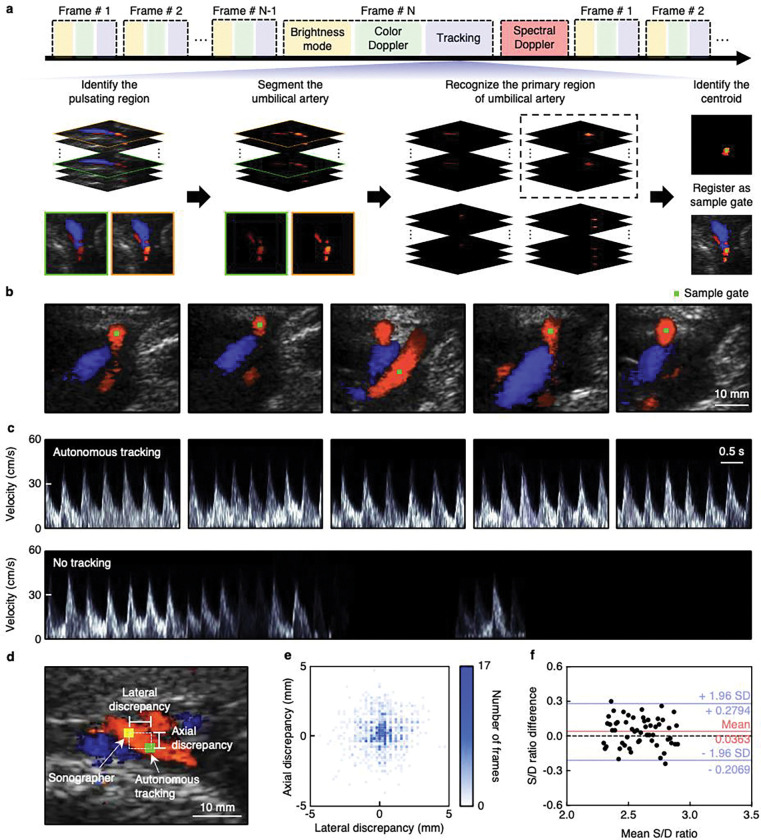
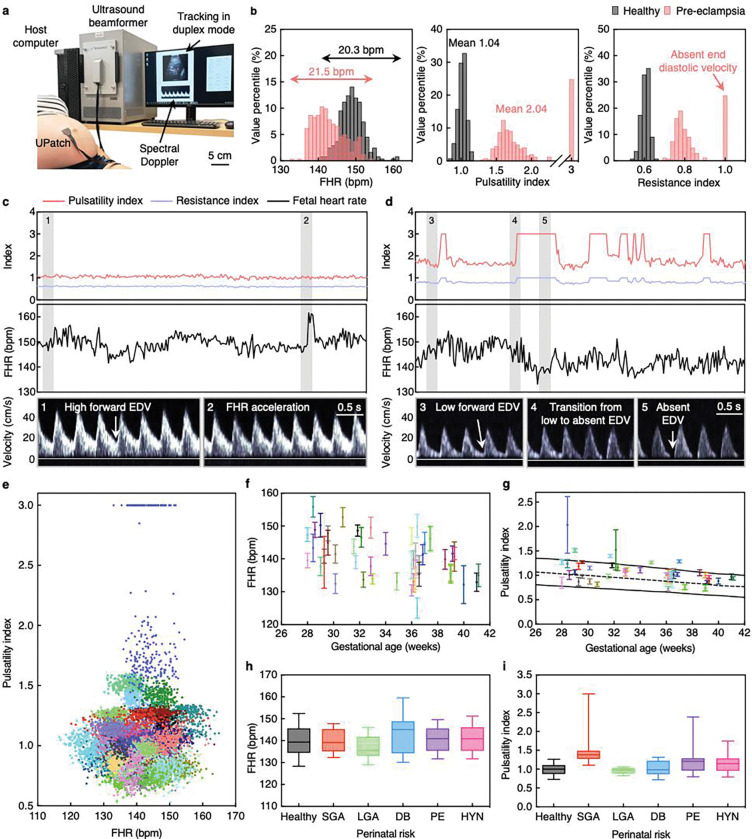
The rapid and complex nature of fetal development requires meticulous prenatal monitoring to ensure optimal pregnancy outcomes1. Cardiotocography, which continuously records the fetal heart rate and uterine contractions, often leads to inaccurate diagnoses and unnecessary interventions2. Ultrasonography is a cornerstone of fetal monitoring and diagnosis, but it is highly dependent on specialized sonographers, limiting its availability3. Additionally, current ultrasound methods provide only snapshot evaluations4. Even in very high-risk pregnancies, it is rare to have fetal ultrasound assessments more than once per day5. Here we report a wearable ultrasound patch (UPatch) for continuous and autonomous fetal monitoring. The UPatch can acquire anatomical structures and blood flow velocities, with signal qualities comparable to those of handheld clinical ultrasound devices. Real-time image segmentation allows the autonomous tracking of target vessels and thus the acquisition of continuous blood flow spectra during fetal and maternal movements without a sonographer. We validated the UPatch accuracy on 62 pregnancies, and the continuous monitoring data on 52 pregnant women aligned with stratified perinatal conditions, including healthy, small for gestational age, large for gestational age, gestational diabetes, pre-eclampsia, and gestational hypertension. The UPatch introduces new capabilities for prenatal care and offers critical evidence for studying fetal complications in high-risk pregnancies.
Conflict of interest statement
Competing interests S.X. is a cofounder of Softsonics LLC. A.T.P. is a Senior Scientific Advisor of Intelligent Ultrasound Ltd. All other authors declare no competing interests.
Figures
References
-
- Rouse D. J. Antepartum fetal surveillance ACOG practice bulletin, number 229. Obstet Gynecol 137, E116–E127 (2021). - PubMed
-
- Marzbanrad F., Stroux L. & Clifford G. D. Cardiotocography and beyond: a review of one-dimensional Doppler ultrasound application in fetal monitoring. Physiological Measurement 39, 08TR01 (2018).
-
- Chudleigh T., Smith A. & Cumming S. Obstetric & Gynaecological Ultrasound: How, Why and When. (Elsevier, 2016).
-
- Maulik D. & Lees C. C. Doppler Ultrasound in Obstetrics and Gynecology. (Springer, 2023).
Methods references
-
- Huang Z. et al. Three-dimensional integrated stretchable electronics. Nature Electronics 1, 473–480 (2018).
-
- Wear K. A. & Shah A. Nominal Versus Actual Spatial Resolution: Comparison of Directivity and Frequency-Dependent Effective Sensitive Element Size for Membrane, Needle, Capsule, and Fiber-Optic Hydrophones. IEEE Transactions on Ultrasonics, Ferroelectrics, and Frequency Control 70, 112–119 (2023). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
