

The use of heterologous antilymphoid agents in canine renal and liver homotransplantation and in human renal homotransplantation
- PMID: 4163340
- PMCID: PMC2675827
Item in Clipboard
The use of heterologous antilymphoid agents in canine renal and liver homotransplantation and in human renal homotransplantation
Surg Gynecol Obstet.
1967 Feb.
No abstract available
Figures
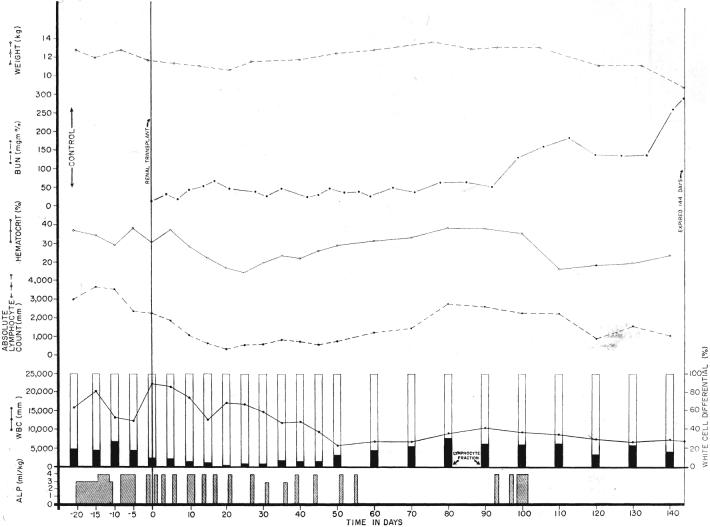
Course of a dog after renal homotransplantation, employing antilymphoid plasma (ALP) for immunosuppression. Note the weight loss and anemia caused by both an early and late course of therapy. Rejection was slow to occur after cessation of treatment. Note the minimal change in the lymphocyte count when the plasma was given during the preoperative period.
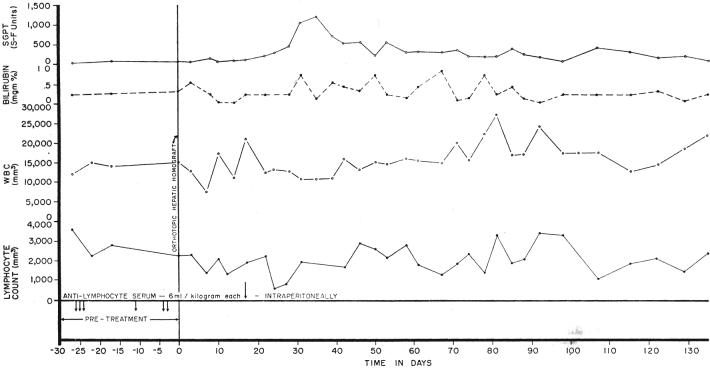
A dog which received an orthotopic liver homograft after 6 intraperitoneal injections of antilymphoid serum (ALS). No postoperative therapy was ever given. Note that the lymphocyte count was little changed. The dog is still alive.
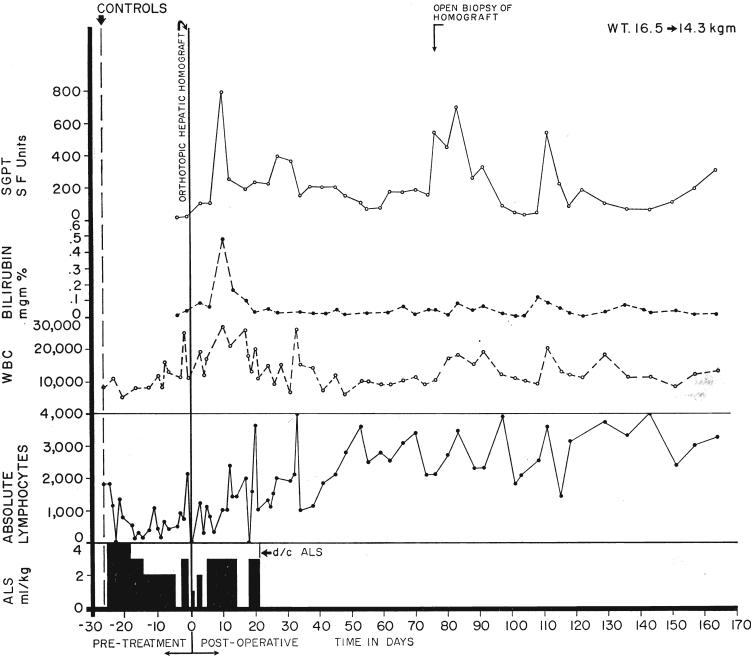
A chronically surviving dog which was treated before and for 20 days after orthotopic liver transplantation with intraperitoneal antilymphoid serum (ALS). Note the pronounced lymphocytosis late in the postoperative period. The animal is in excellent health after almost 6 months.
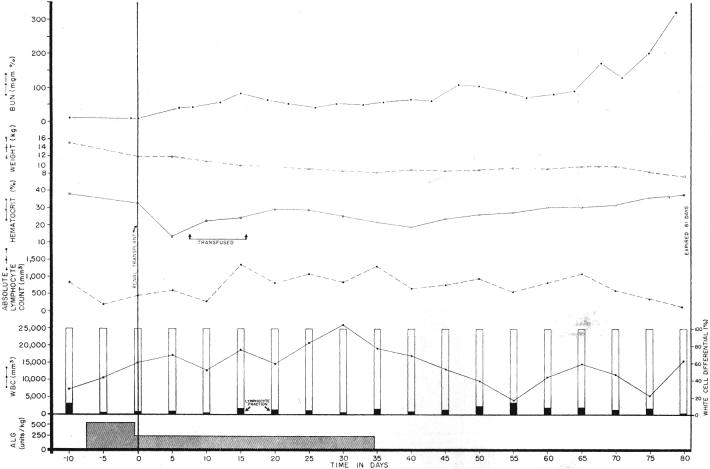
Potentiation of canine renal homograft survival with immunosuppression by antidoglymphoid globulin (ALG). Although the lymphocyte differential fraction was reduced, the total white count was increased and the absolute lymphocyte count was higher postoperatively than during the control period. The early postoperative anemia was apparently due to operative blood loss. Note the slow rejection after cessation of therapy.
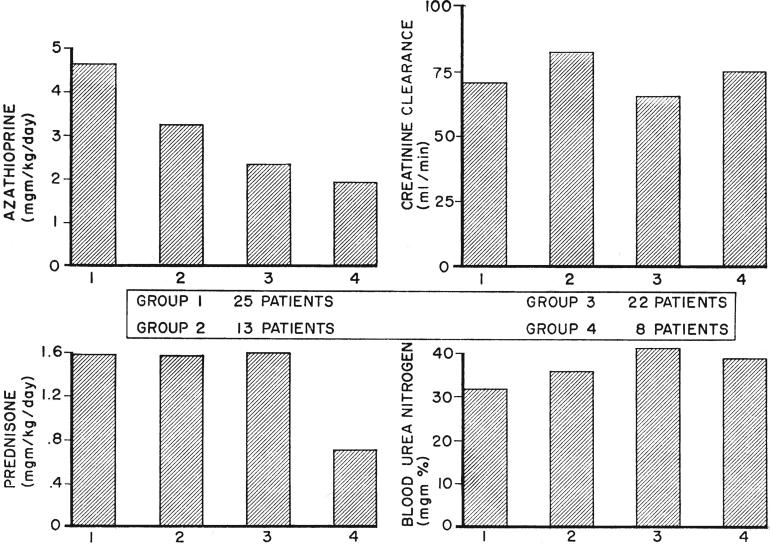
Variations in immunosuppression and renal function during the first 63 postoperative days in 4 successive groups of patients who received kidneys from blood relatives. Since the blood urea nitrogen and creatinine clearance were not determined each day, these were compiled on a weekly basis. Those in series 4 received adjuvant therapy with antilymphoid globulin. Note the drastic reduction in average prednisone dose which was achieved in these patients without significant loss of renal function. The progressive diminution of azathioprine dosage in the succeeding series is evident.
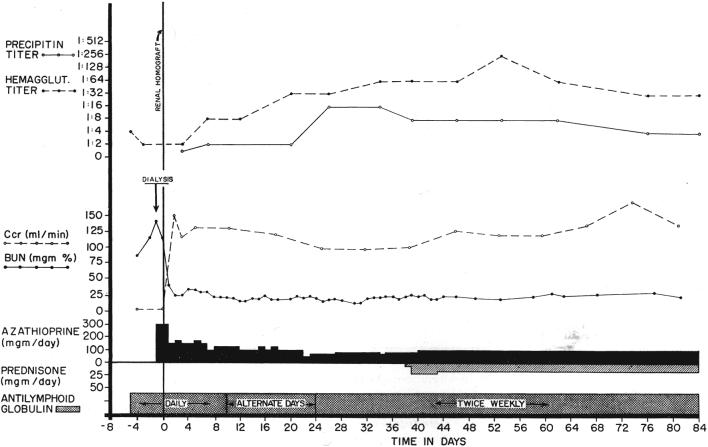
Course of a patient treated before and after renal homotransplantation with antilymphoid globulin. No rejection occurred. Note the rises in precipitin and hemagglutinin titers, findings which prompted institution of prednisone therapy. These titers subsequently fell. This patient had a good antigen match with his sibling donor.
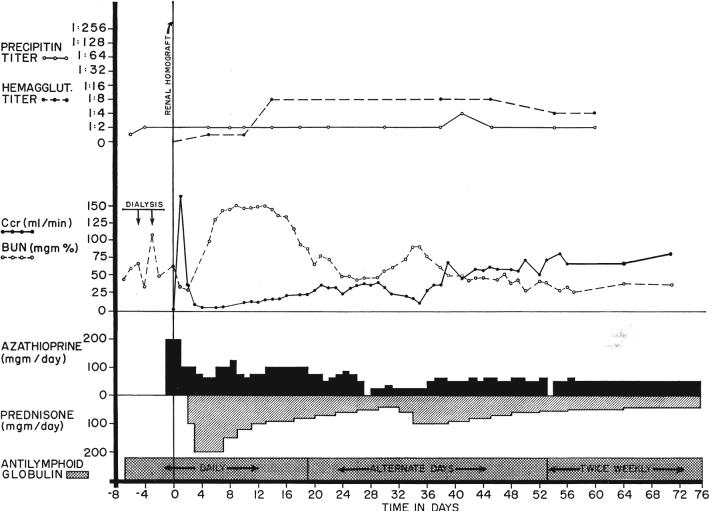
The course of the only patient who had a moderately severe rejection among the 8 treated from the beginning with antilymphoid globulin (ALG). The young woman, who had a very poor Terasaki antigen match with her fraternal donor, required large doses of steroids which may have contributed to the relative lack of response in the precipitin and leukoagglutinin titers.
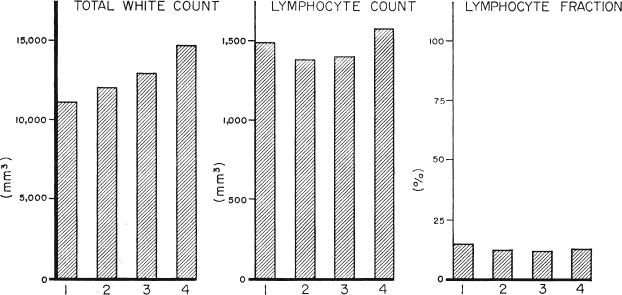
Effect of different immunosuppressive regimens upon peripheral white cells. The 4 series are in the same order as in Figure 5. Group 4 received adjuvant therapy with antilymphoid globulin. The higher average total white cell count in the later series was apparently due to greater conservatism with the use of azathioprine. The differences in lymphocyte per cents and total counts were not significant.
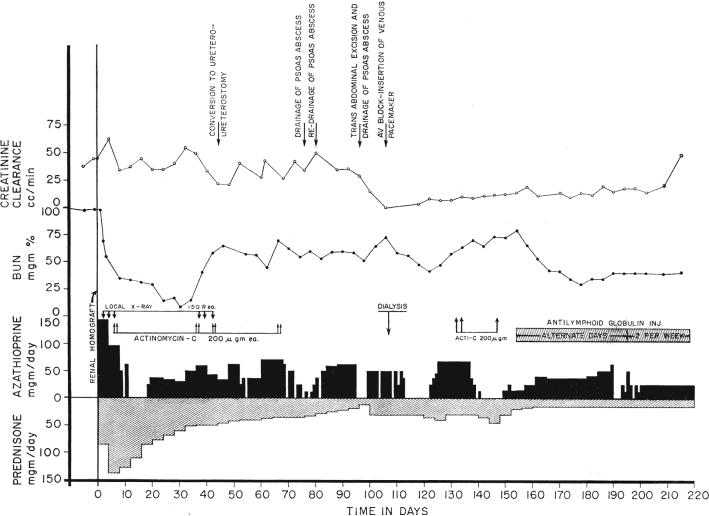
Course of patient with a failing renal homograft who was treated late with antilymphoid globulin. During the first 4 postoperative months, there were several potentially lethal postoperative complications which were made more grave by the need for heavy steroid therapy. Efforts to reduce the prednisone dosage resulted in deterioration of renal function. After institution of antilymphoid globulin therapy, renal function slightly improved despite a rapid decrease of the steroid doses.
References
-
- Abaza H, Nolan B, Watt J, Woodruff MFA. The effect of antilymphocytic serum on the survival of renal homotransplants in dogs. Transplantation. 1966;4:618. - PubMed
-
- Gray JG, Monaco AP, Russell PS. Surgical Forum, Clinical Congress 1964. XV. American College of Surgeons; Chicago: 1964. Heterologous mouse antilymphocyte serum to prolong skin homografts. p. 142. - PubMed
-
- Gray JG, Monaco AP, Wood ML, Russell RS. Studies on heterologous antilymphocyte serum in mice–I, in vitro and in vivo properties. J. Immun., Bait. 1966;96:217. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources