

Acute pancreatitis and hyperamylasemia in renal homograft recipients
- PMID: 4557978
- PMCID: PMC2964057
- DOI: 10.1001/archsurg.1972.04180080021004
Acute pancreatitis and hyperamylasemia in renal homograft recipients
Abstract
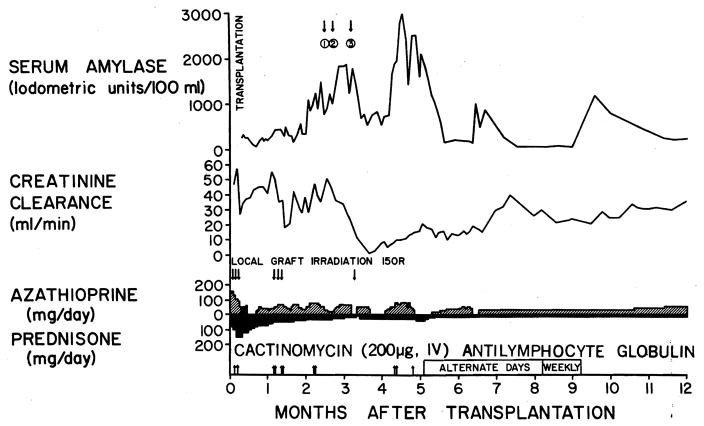
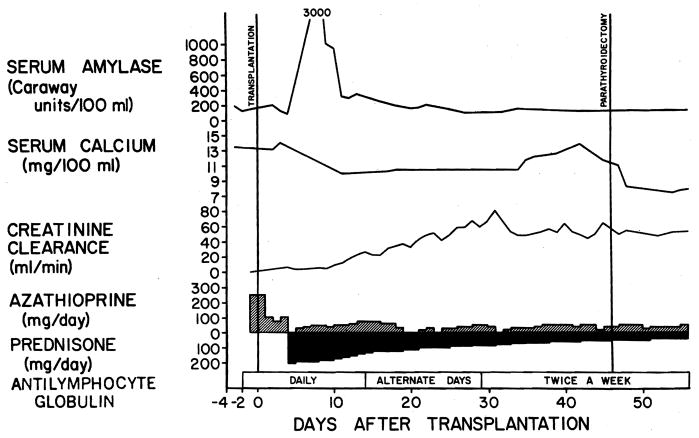
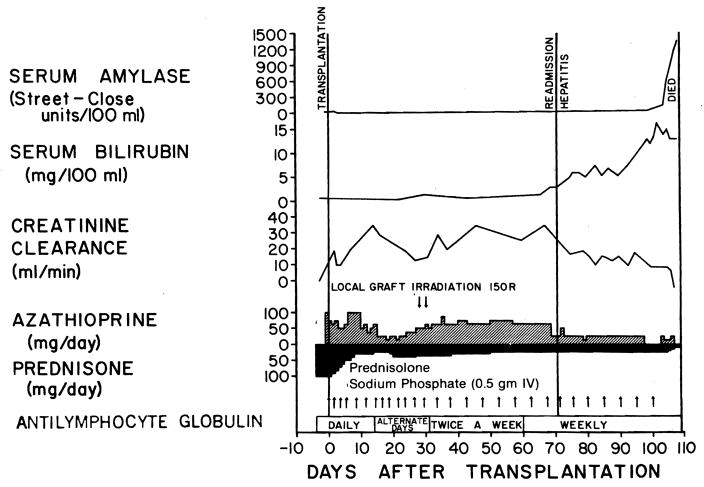
In a series of 301 renal homograft recipients, 17 (5.6%) had acute pancreatitis at some time after transplantation. Eleven of these patients died, for a mortality of 64.7%. In each instance, pancreatitis was a major factor in a complex chain of lethal events to which immunosuppression invariably contributed. An additional 43 patients (14.3%) developed asymptomatic hyperamylasemia after transplantation and, undoubtedly, some of these recipients also had pancreatitis. The factors causing pancreatitis in the renal transplantation patient include uremia, hyperparathyroidism, pancreatic injury by drugs, infections resulting from chronic immunosuppression, gallstones, and operative trauma to the pancreas. In cases of preexisting pancreatitis, transplantation is not necessarily precluded, but efforts should be made to find a specific cause of the pancreatitis and take corrective measures, such as biliary tract surgery or parathyroidectomy if indicated, in advance of transplantation.
Figures
References
-
- Hill RB, Jr, Dahrling BE, II, Starzl TE, et al. Death after transplantation. An analysis of sixty cases. Amer J Med. 1967;42:327–334. - PubMed
-
- Starzl TE. Experience in Renal Transplantation. Philadelphia: WB Saunders Co; 1964.
-
- Tilney NL, Collins JJ, Jr, Wilson RE. Hemorrhagic pancreatitis. A fatal complication of renal transplantation. New Eng J Med. 1966;274:1051–1057. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
