

Chronic renal homograft function: correlation with histology and lymphocyte antigen matching
- PMID: 4862761
- PMCID: PMC2965524
- DOI: 10.1016/0002-9343(67)90242-2
Chronic renal homograft function: correlation with histology and lymphocyte antigen matching
Abstract
Renal function was studied in twenty-nine of thirty-four surviving renal allograft recipients from an initial group of sixty-four patients two years after transplantation. Mean clearances of inulin and PAH were, respectively, greater than and equal to half the donors’ initial predicted clearances. Minimum urine osmolality during water diuresis was greater, and maximum urine osmolality during hydropenia was less than normal, an effect attributable partly to enhanced solute load in a single transplanted kidney.
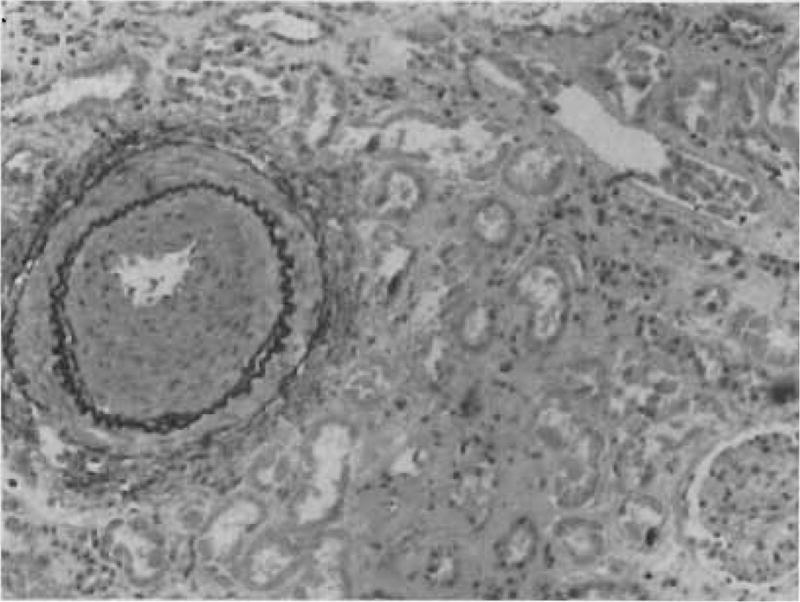
Patients with compatible donor-recipient lymphocyte antigens demonstrated statistically better function than those with one or more incompatibilities, although there was a definite degree of overlap between the two groups. In contrast, little correlation could be demonstrated between the cumulative histopathology and renal clearances.
Renal function in patients with compatible donors was statistically greater than half the donors’ initial predicted function. Serial increase in renal clearances was documented in one patient with a compatible donor. Serial decreases were demonstrated in two patients with incompatible donors. These findings suggest that hypertrophy of the denervated, transplanted kidney occurs when immune reaction is minimal.
Figures







References
-
- Murray JE, Gleason R, Bartholomay A. Fourth report of the human kidney transplant registry. Transplantation. 1965;3:684. - PubMed
-
- Starzl TE. Experience in Renal Transplantation. Philadelphia: W. B. Saunders Co; 1964.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
