

Cyclophosphamide and whole organ transplantation in human beings
- PMID: 4940540
- PMCID: PMC2762737
Item in Clipboard
Cyclophosphamide and whole organ transplantation in human beings
Surg Gynecol Obstet.
1971 Dec.
No abstract available
Figures
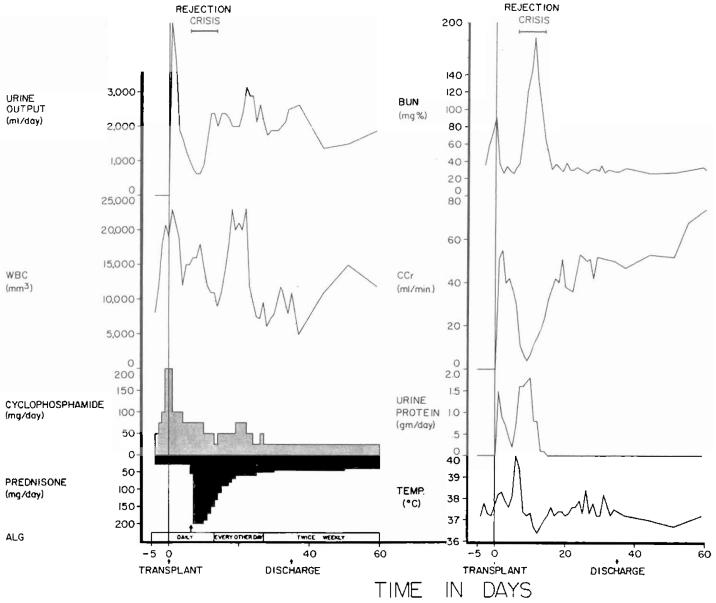
The first 60 days after the transplantation of a kidney from a mother to her 14 year old daughter. The rejection crisis after a week was the most severe observed in the intrafamilial cyclophosphamide series, with the exception of two hyperacute rejections. However, it was easily and completely reversed. Note that leukopenia was never produced by the daily doses of cyclophosphamide that were usually between 0.5 to 1 milligram per kilogram per day. ALG, Horse antilymphocyte globulin; BUN, blood urea nitrogen level; CCr, creatinine clearance; WBC, white blood cell count; and arrow, 625 milligrams of methyl prednisolone intravenously.
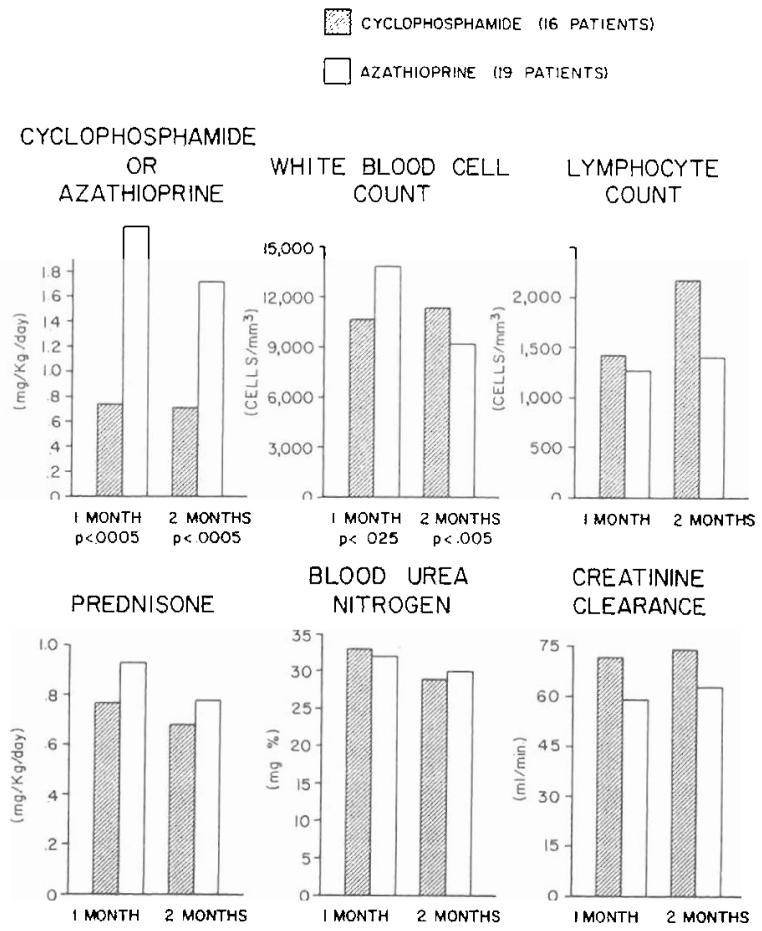
Drug doses and laboratory measurements at the end of one and two months in patients given either cyclophosphamide or azathioprine. All these recipients of kidneys donated by blood relatives were also treated with prednisone and horse antilymphocyte globulin. The p values are noted only for differences that were statistically significant.
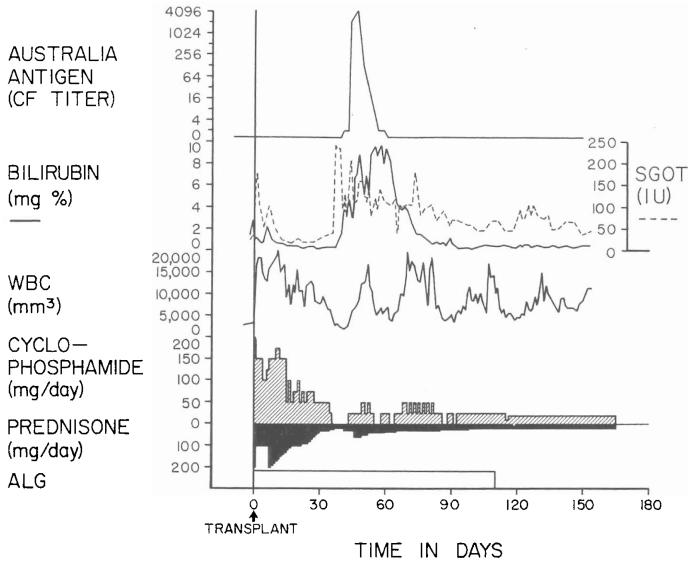
Triple drug therapy with cyclophosphamide, prednisone, and horse antilymphocyte globulin in a 15 year old male who had an orthotopic liver transplantation for Wilson's disease. Rejection has never been diagnosed postoperatively. The temporary deterioration in hepatic function in the second postoperative month was accompanied by Australia antigenemia and consequently was thought to be a manifestation of serum hepatitis. ALG, Horse antilymphocyte globulin; CF, complement fixation; SGOT, serum glutamic oxalacetic transaminase in international units; and WBC, white blood cell count.
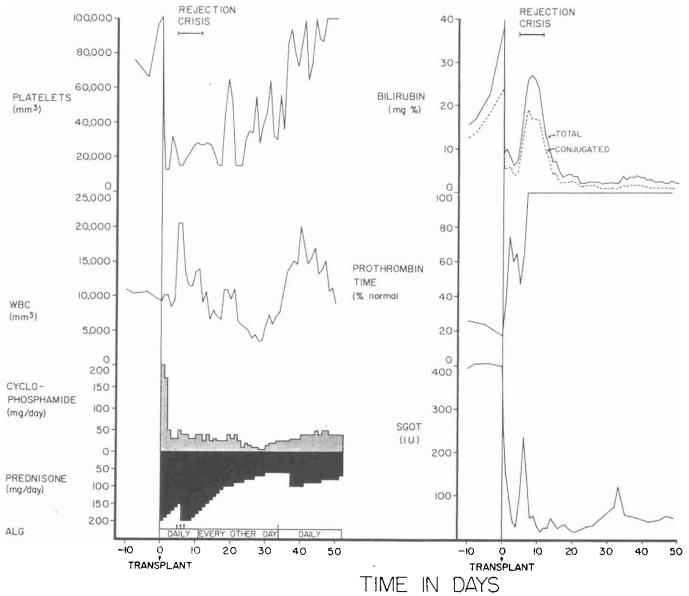
The early course of a 52 year old male who had total liver replacement as treatment for a hemangioendothelial sarcoma. This rare liver tumor usually causes death from fulminating hepatic failure in a few weeks or months, but it does not commonly metastasize. After transplantation, there was a severe rejection crisis. The protracted thrombocytopenia postoperatively is often noted after liver transplantation and is probably due to thrombocyte sequestration in the homograft. ALG, Horse antilymphocyte globulin; SGOT, serum glutamic oxalacetic transaminase in international units; and arrow, 625 milligrams of methyl prednisolone intravenously.
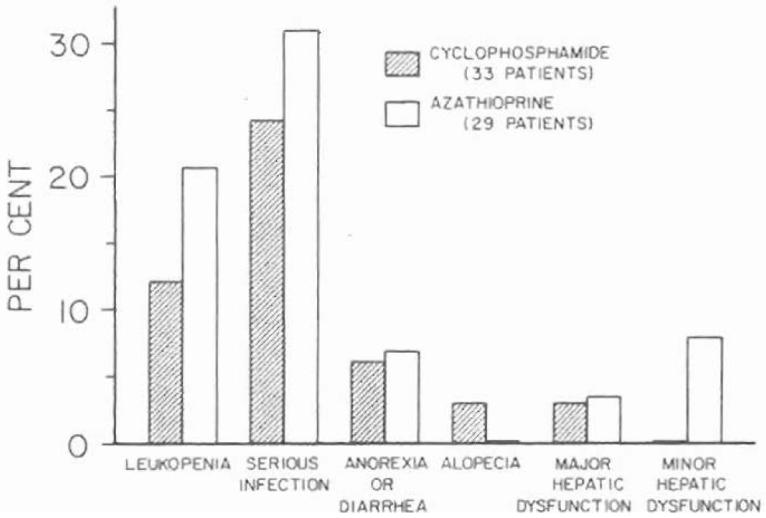
Incidence of toxicity in the first two months of treatment of renal homograft recipients with cyclophosphamide versus azathioprine. At the dosages used, there was little obvious difference between the two agents. The one patient under cyclophosphamide therapy in whom major hepatic dysfunction developed had a proved attack of acute serum hepatitis, Australia antigen positive.
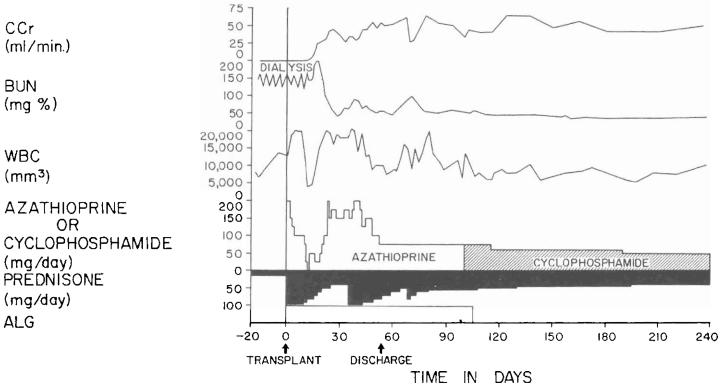
The consecutive use of azathioprine and cyclophosphamide after cadaveric renal homotransplantation in a 20 year old male is charted. The change to cyclophosphamide was made because of dissatisfaction with the early postoperative course. There was slow improvement in the subsequent convalescence, but, retrospectively, there is no reason to believe that this might not have occurred even without making the drug switch. The globulin injections were daily for ten days, every other day for 20 days, and twice a week until they were discontinued because of anaphylactic reactions. ALG, Horse antilymphocyte globulin; BUN, blood urea nitrogen level; CCr, creatinine clearance; and WBC, white blood cell count.
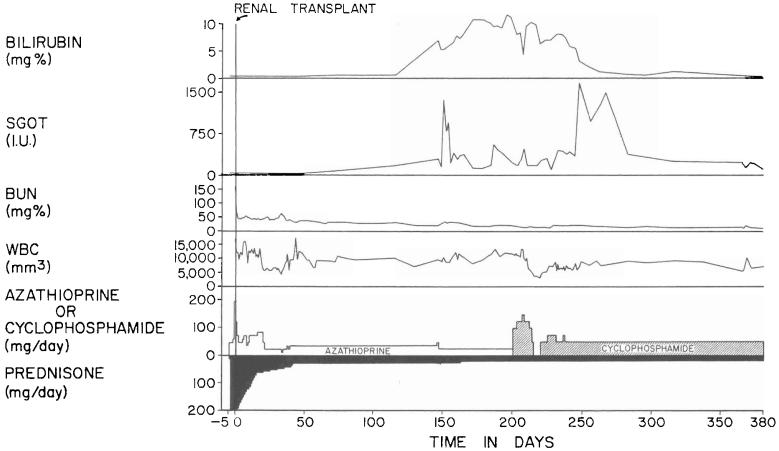
The course of a 17 year old female in whom azathioprine was stopped because of the suspicion of hepatotoxicity. Multiple Australia antigen tests for serum hepatitis were negative. Note the recession of jaundice after the substitution of cyclophosphamide for azathioprine. BUN, blood urea nitrogen level; SGOT, serum glutamic oxalacetic transaminase in international units; and WBC, white blood cell count.
References
-
- BUCKLEY CE, DURHAM NC, GILLS JP. Cyclophosphamide therapy of peripheral uveitis. Arch. Intern. Med. 1969;124:29. - PubMed
-
- ELION GP. Biochemistry and pharmacology of purine analogues. Fed. Proc. 1967;26:898. - PubMed
-
- FOSDICK WM, PARSONS JL, HILL DF. Long-term cyclophosphamide (CP) therapy in rheumatoid arthritis; a progress report, six years' experience. Arthritis Rheum. 1969;12:663. - PubMed
-
- Fox M. Suppression of tissue immunity by cyclophosphamide. Transplantation. 1964;2:475. - PubMed
-
- GOODWIN WE, KAUFFMAN JJ, MIMS MM, TURNER RD, GLASSOCK R, GOLDMAN R, MAXWELL MM. Human renal transplantation—I, clinical experiences with 6 cases of renal homotransplantation. J. Urol. 1963;89:13. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources