

doi: 10.1001/archsurg.1966.01330010109014.
Auxiliary liver transplantation: effect of host portacaval shunt. Experimental and clinical observations
- PMID: 5327725
- PMCID: PMC2962590
- DOI: 10.1001/archsurg.1966.01330010109014
Item in Clipboard
Auxiliary liver transplantation: effect of host portacaval shunt. Experimental and clinical observations
Arch Surg.
1966 Jul.
No abstract available
Figures
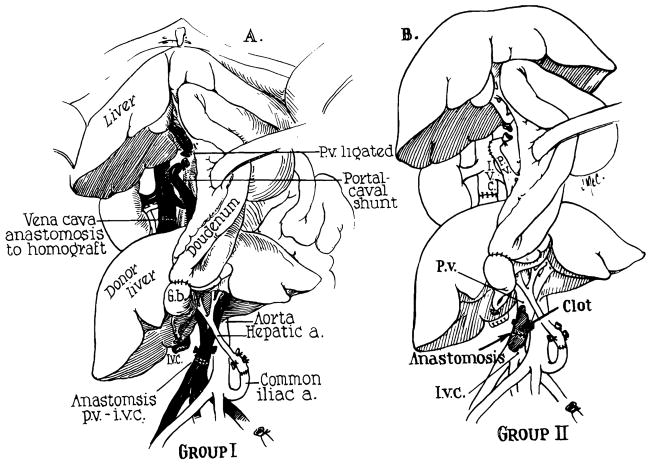
Experimental design of auxiliary canine homotransplantation of the liver, in conjunction with host portacaval shunt. (A) Group 1 Series: Note that the homograft receives a double blood supply, the portal inflow being of systemic venous origin. Except for the host portacaval shunt, the procedure is essentially that described by Welch?. (B) Group 2 Series: In these dogs the portal venous anastomosis clotted. Thus, both the host liver and homograft received only an arterial blood supply.
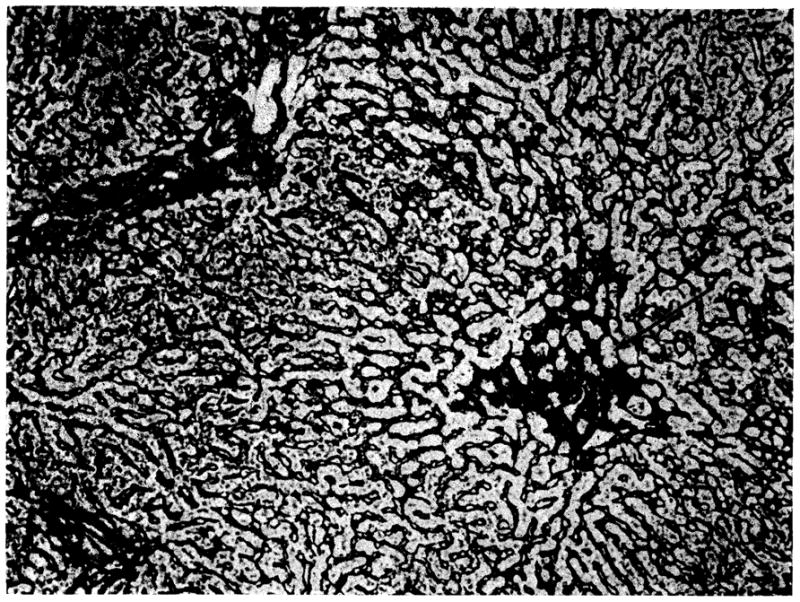
Own liver of dog 8 from group 1. Atrophy of the centrilobular hepatocytes has permitted collapse of the central part of the lobular reticulin framework (arrow) (reticulin stain, × 80).
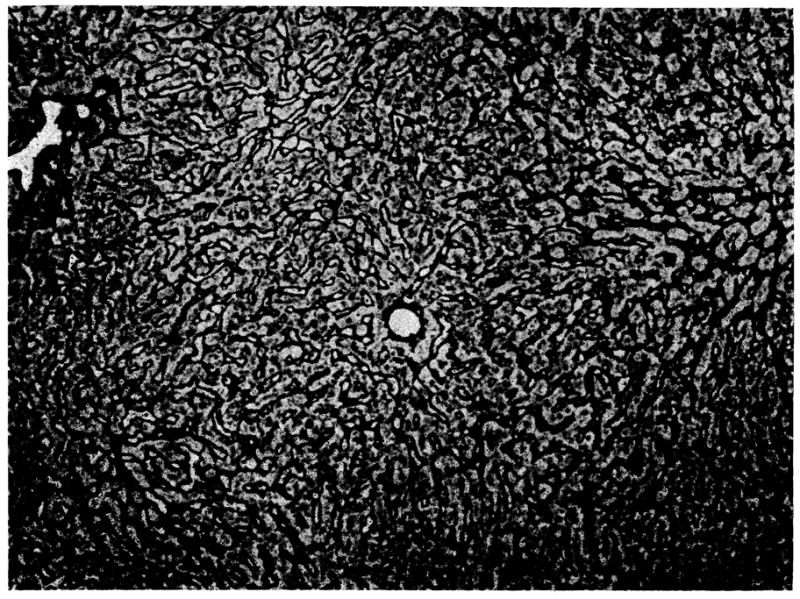
Biopsy at 35 days of auxiliary hepatic homograft from dog 8 (group 1). The lobular reticulin framework is normal. Twenty-eight days later this liver showed increased central and portal connective tissue and some pseudolobules (reticulin stain, × 80).
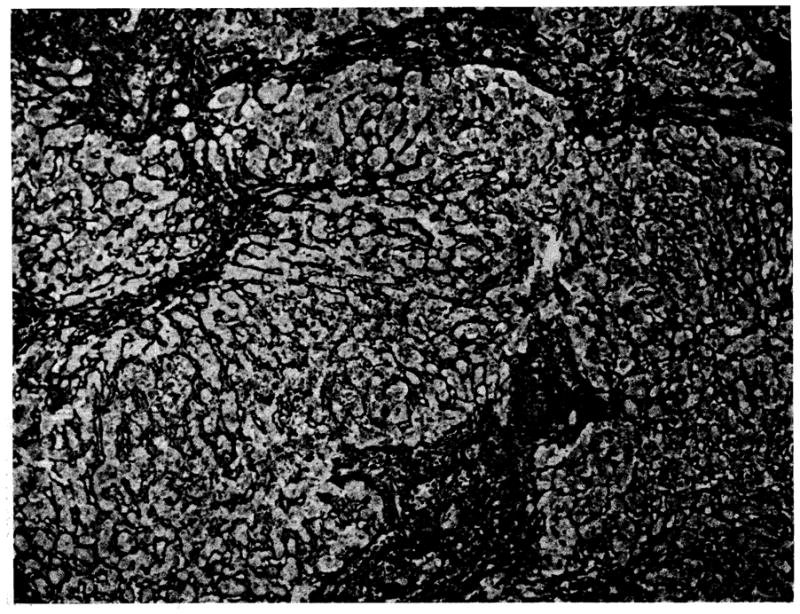
Biopsy at 35 days of auxiliary hepatic homograft from dog 1 (group 2). The normal lobular architecture has been disrupted by bands of connective tissue which link portal tracts and some central veins. There is increased reticulin in the portal areas and around the central veins (reticulin stain, × 80).
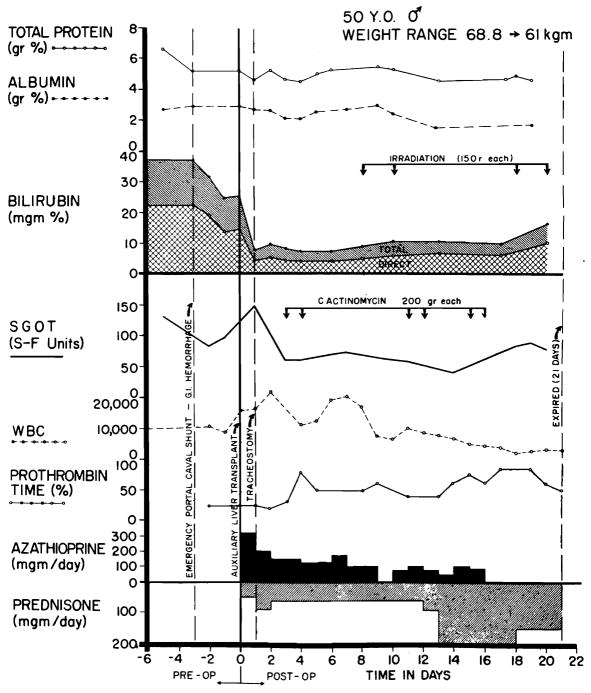
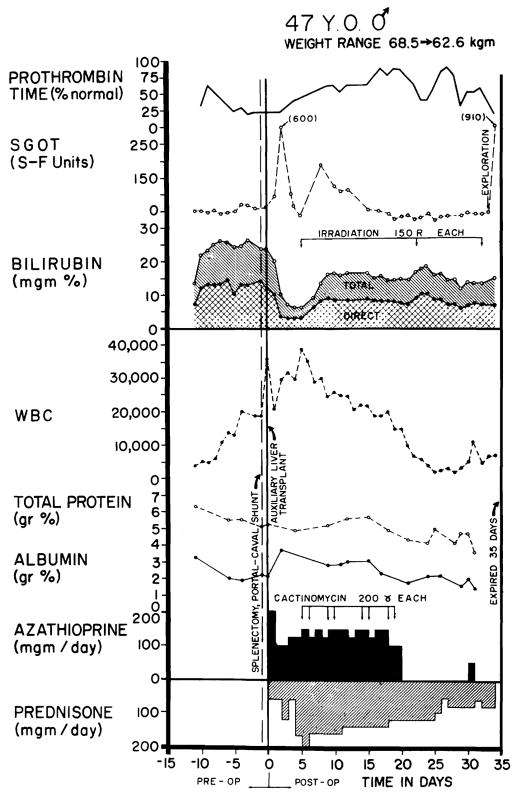
Clinical course of patient 1. Note the sharp fall in serum bilirubin after auxiliary homotransplantation, as well as the sustained improvement in prothrombin time. Later, the bilirubinemia slowly increased at a time when rejection was thought to be present. Severe leukopenia ensued late in the second week and necessitated withdrawal of azathioprine.
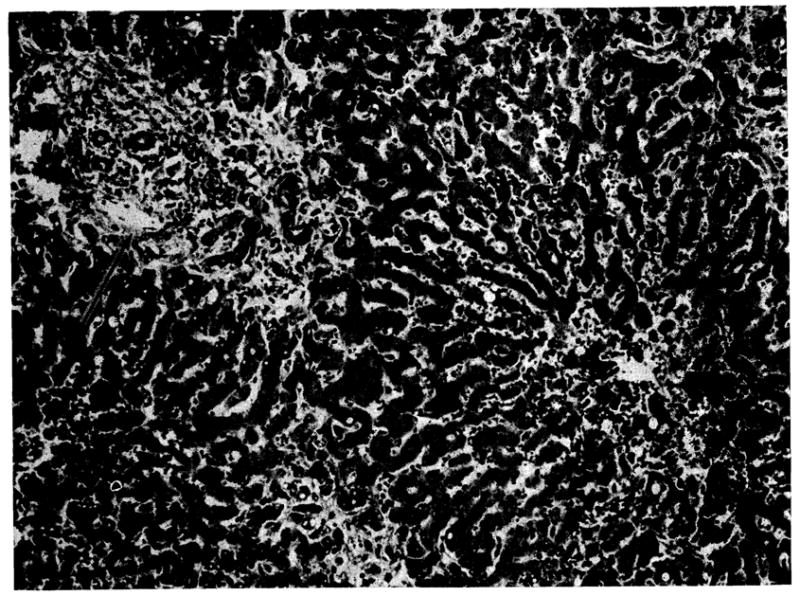
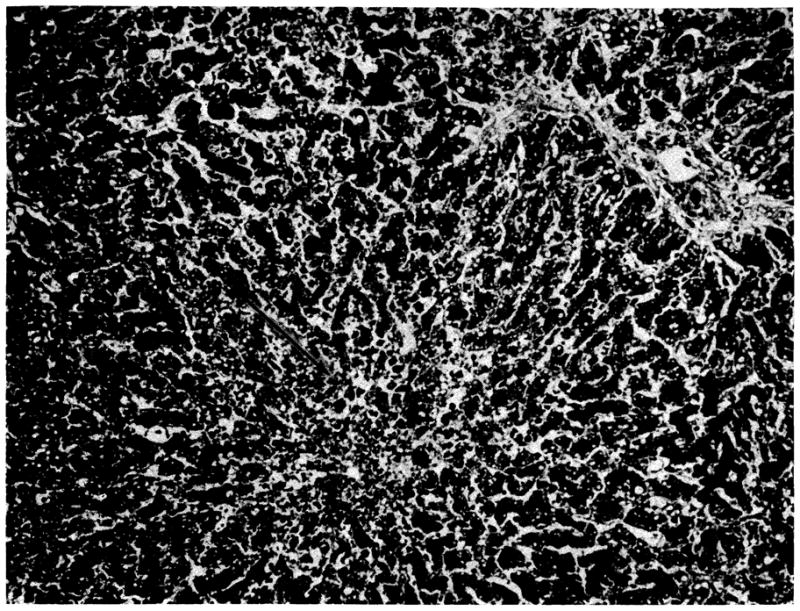
Auxiliary human hepatic homograft 22 days after transplantation (case 1). The portal tract (arrow) is infiltrated by mononuclear cells and several of the smaller bile ducts contain casts. There is central cholestasis, excess lipofuscin in the central hepatocytes, and atrophy of the liver cells adjacent to the central vein (lower right) (hematoxylin and eosin, ×80).
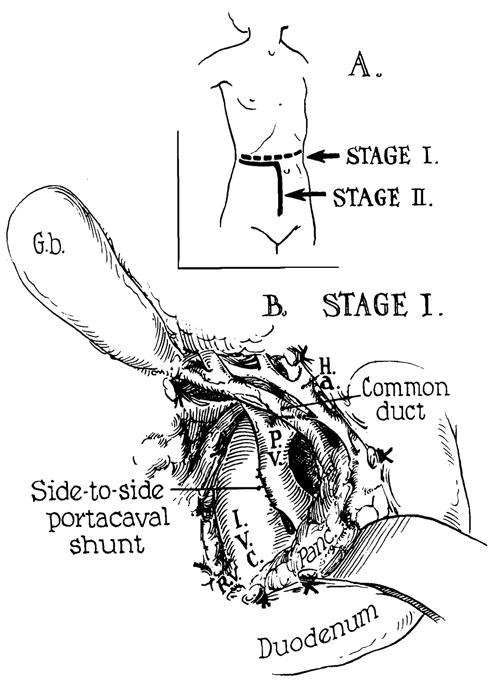
Human auxiliary liver homotransplantation. At the first stage, portacaval shunt was performed transabdominally for emergency control of variceal hemorrhage. Stage 2 was the actual transplantation, one day later. (A) Incisions: Note that part of the stage 1 incision was reused for stage 2. (B) Completed side-to-side portacaval shunt.
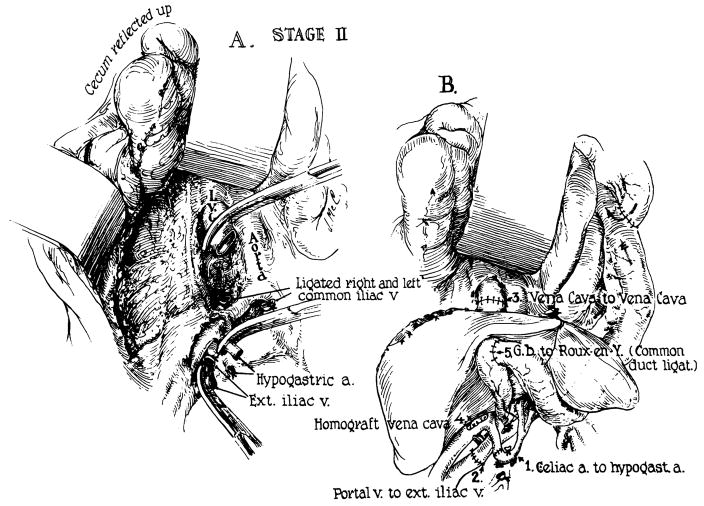
Actual auxiliary transplantation (Stage 2). (A) Prepared operative field before receipt of homograft. (B) Completed operation. Note that the right external iliac vein provides the portal venous inflow. Hepatic venous outflow is into the transected vena cava.
Clinical course of patient 2. As in case 1 (Fig 5) the early rise in SGOT is probably ascribable to ischemic injury to the homograft. Note the abrupt fall in serum bilirubin and the improvement in prothrombin time. Rejection was diagnosed on day 4, after which serum bilirubin rose but never to the preoperative level. The inexorable leukopenia which began during the third post-operative week was apparently the most important cause of ultimate failure; the patient died of sepsis.
Auxiliary human hepatic homograft 34 days after transplantation (case 2). The centrilobular hepatocytes are necrotic (arrow) and there are fat droplets in the liver cells in the rnidzonal and peripheral parts of the lobule. There is no cellular infiltration (hematoxylin and eosin, ×80).
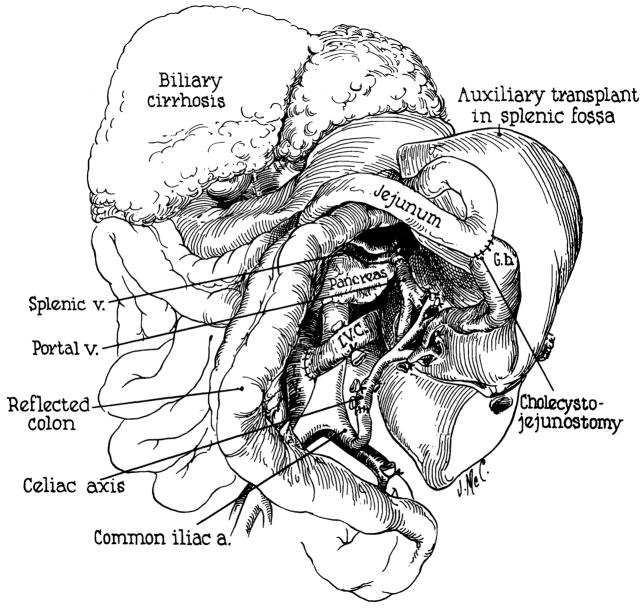
Technique used for attempted transplantation in case 3. Note that the homograft is facing medially. The splenic vein and common iliac artery are anastomosed to the homograft portal vein and hepatic artery, respectively. Note also the angulation near the origin of the left cornmon iliac artery. This was responsible for the technical failure of the transplant.
References
-
- Marchioro TL, et al. The Specific Role of Splanchnic Venous Blood in the Maintenance of Hepatic Structure and Function. to be published.
-
- Spector WD, editor. Handbook of Biological Data. Philadelphia: W. B. Saunders Co; 1956.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
