

Left hepatic trisegmentectomy
Surg Gynecol Obstet.
1982 Jul.
No abstract available
Figures
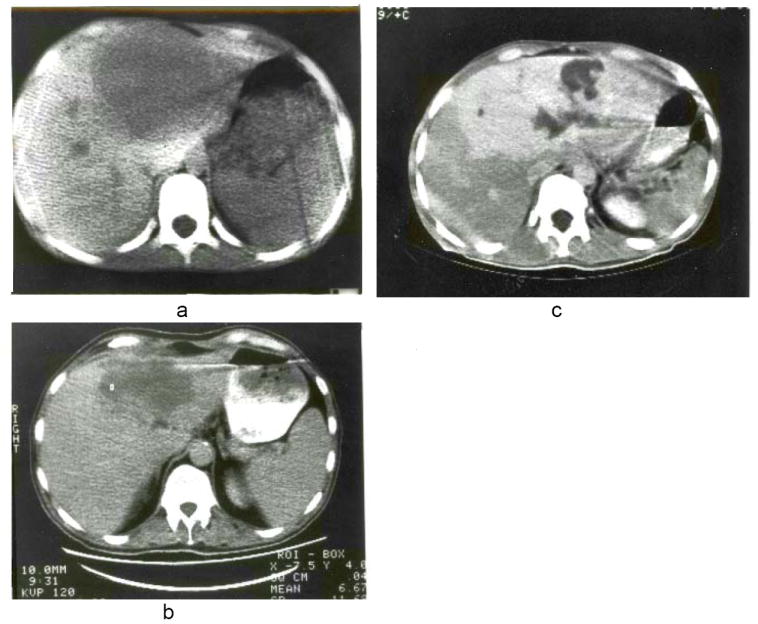
a, b and c, Scans of liver in Patients 1, 2 and 3 obtained with computerized axial tomography. Note predominant involvement of the left lobes but with extension into the anterior segments of the right lobes. c, The white appearance of the lesion was due to the prior injection of contrast medium intravenously.
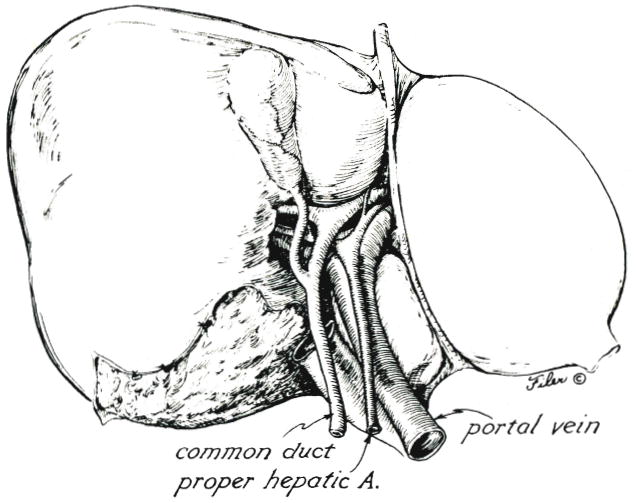
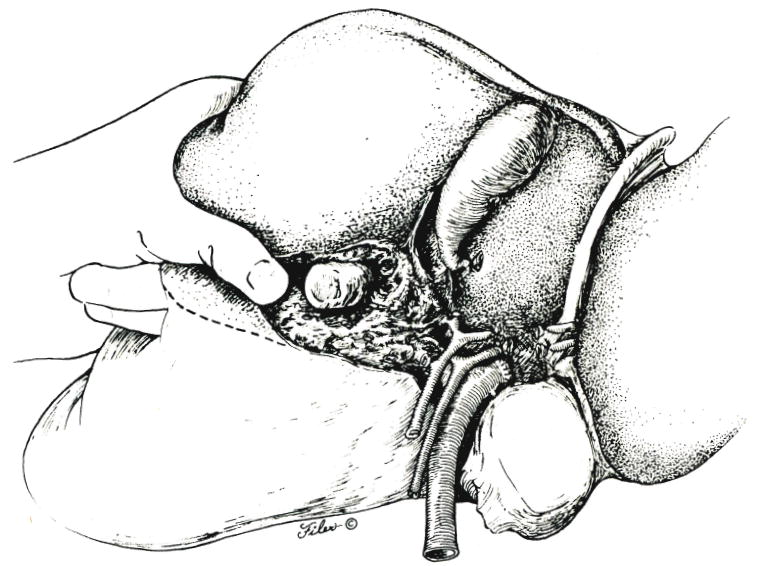
Structures of the hilus of the liver.
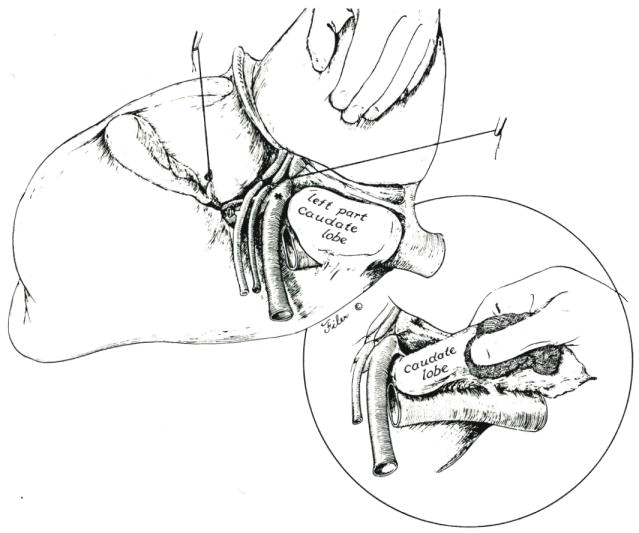
Exposure of the left hilar structures is accomplished by retracting the lateral segment of the left lobe anteriorly and to the right. Branches to the left portion of the caudate lobe are preserved if the latter liver fragment is to be retained. Otherwise, the left structures are ligated at their origin, *. Inset, If the left portion of the caudate lobe is removed, it must be dissected from the retrohepatic inferior vena cava, and several small hepatic veins must be ligated.
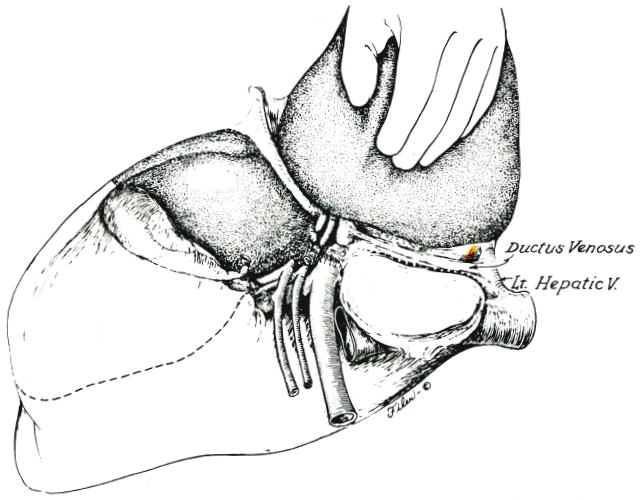
Line of incision into the capsule of the liver along obliterated ductus venosus which is used if the left portion of the caudate lobe is retained. Alternatively, the line of posterior incision is along the vena cava (Fig. 3, inset) if the caudate fragment is removed. Eventual plane between anterior and posterior segments of the right lobe is shown.
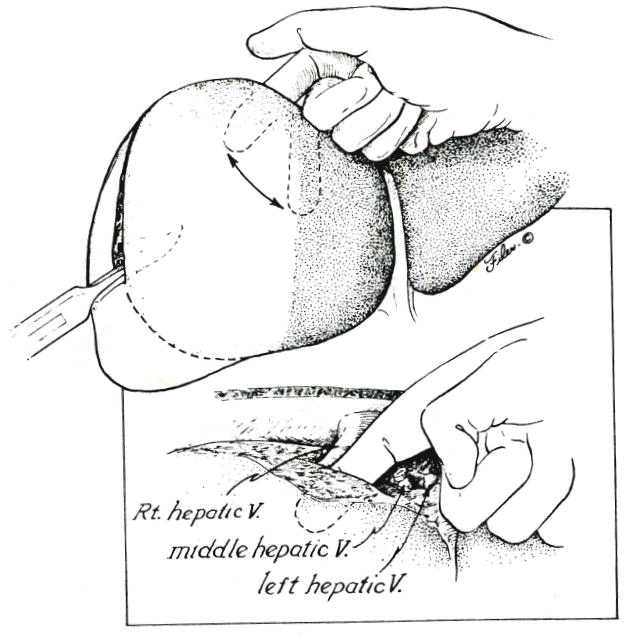
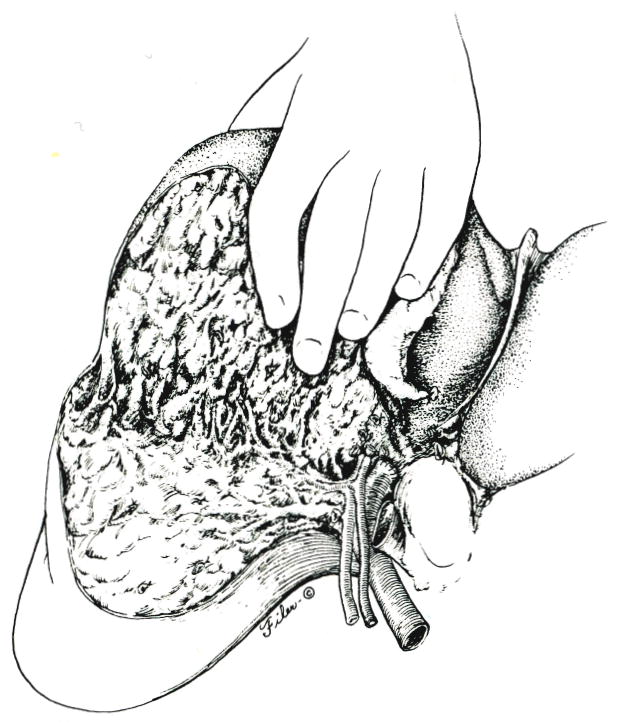
Superior to inferior scalping of the anterior segment of the right lobe. Inset, Note that the dissecting finger is kept anterior to the right hepatic vein, the left and middle hepatic vein having been ligated or sutured.
Further development of plane between the anterior and posterior segments of the right lobe of the liver.
Alternative approach, with which the anterior segment is scalped from the hilus of the liver to the diaphragm.
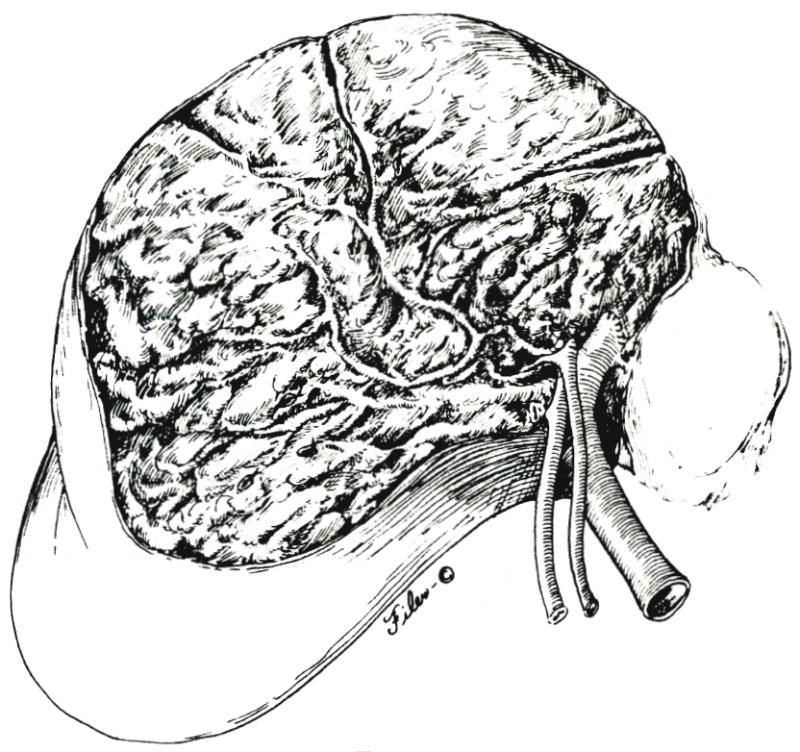
Operative field after removal of specimen.
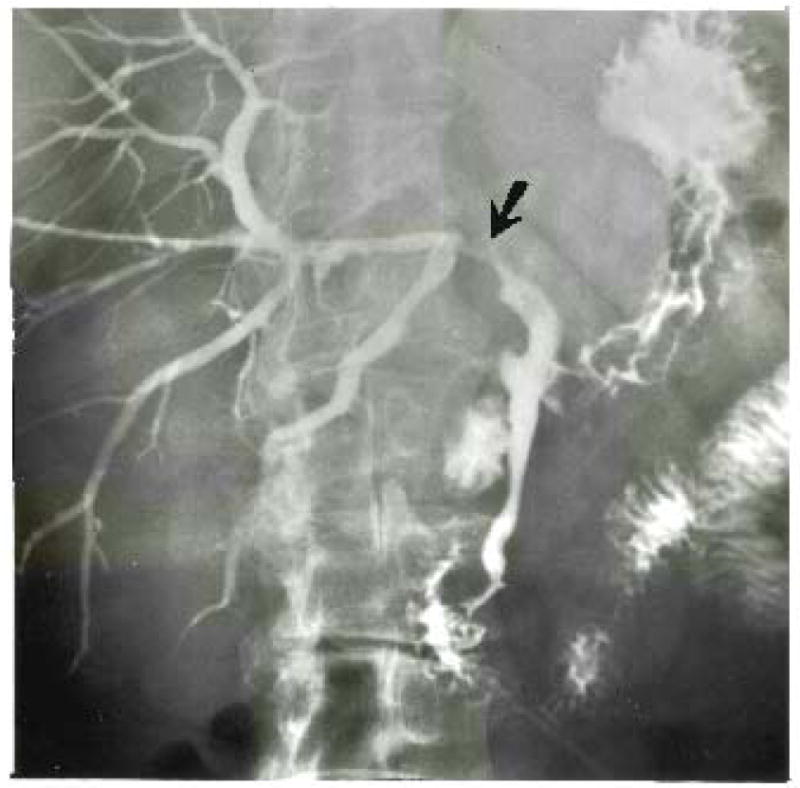
Patient 2. Stricture of right hepatic duct at its termination in the posterior segmental duct. The exposed and denuded duct is susceptible to injury at this location.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical