

Pancreaticoduodenal transplantation in humans
Abstract
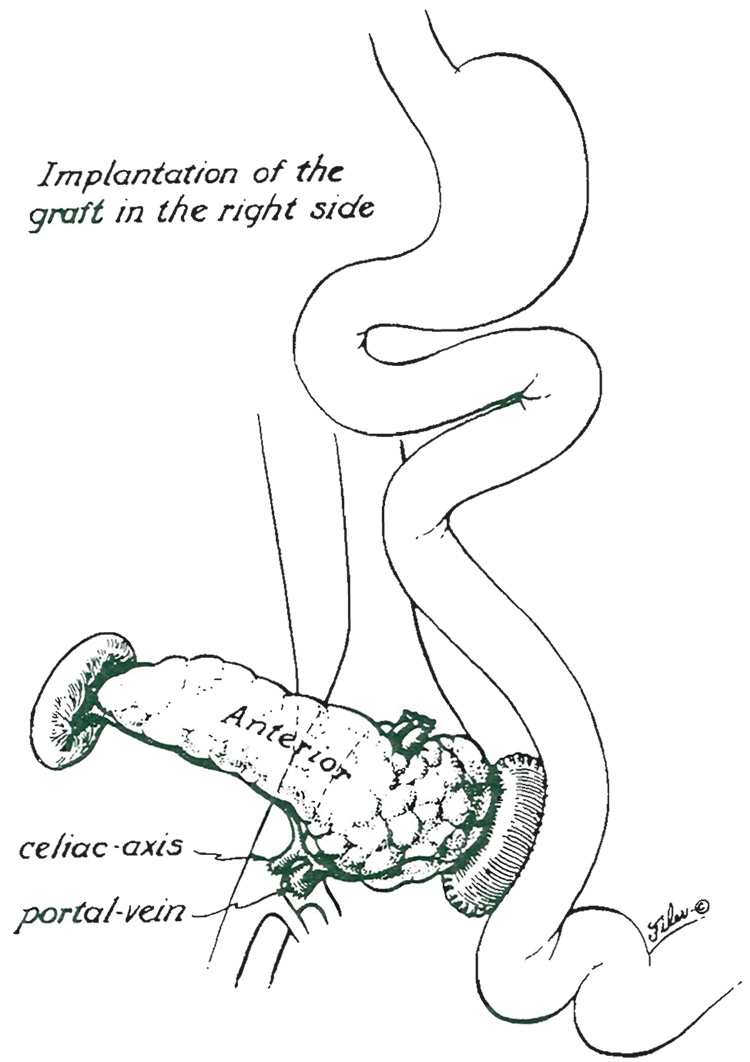
Whole cadaveric pancreata were transplanted to the pelvic extraperitoneal location in four patients with diabetes who previously had undergone successful cadaveric renal transplantation. One graft was lost within a few hours from venous thrombosis but with patient survival. The other three are providing normal endocrine function after two and a half, 11 and 12 months. The exocrine pancreatic secretions were drained into the recipient jejunum through enteric anastomoses. Because mucosal slough of the graft duodenum and jejunum in two patients caused a protein losing enteropathy and necessitated reoperations, we now do the pancreatic transplantation with only a blister of graft duodenum large enough for side-to-side enteroenterostomy. The spleen has been transplanted with the pancreas mainly for technical reasons, and this technique should have further trials in spite of the fact that delayed graft splenectomy became necessary in two recipients to treat graft induced hematologic complications.
Figures




References
-
- Kelly WD, Lillehei RC, Merkel FK, et al. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967;61:827–837. - PubMed
-
- Lillehei RC, Idezuki Y, Feemster JA, et al. Transplantation of stomach, intestines and pancreas; experimental and clinical observations. Surgery. 1961;62:721–741. - PubMed
-
- Sutherland DER. Current status of clinical pancreas and islet transplantation; registry results. Horm. Metab. Res. 1983;13 Suppl.:28–36. - PubMed
-
- Land W, Landgraf R. Segmental pancreatic transplantation, international work shop. Horm. Metab. Res. 1983;13 Suppl.:1–104. - PubMed
-
- Svejgaard A, Ryeer LP. HLA genotype distribution and genetic models of insulin-dependent diabetes mellitus. Ann. Hum. Genet. 1981;45:293–298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical