

Review
doi: 10.1002/hep.1840020516.
Evolution of liver transplantation
- PMID: 6749635
- PMCID: PMC2972731
- DOI: 10.1002/hep.1840020516
Item in Clipboard
Review
Evolution of liver transplantation
Hepatology.
1982 Sep-Oct.
No abstract available
Figures

Yearly number of liver transplantations at the University of Colorado (1963 to 1980) and the University of Pittsburgh (1981 to 1982). Note that retransplantation has been attempted frequently.

Completed orthotopic liver transplantation. (A) Biliary tract reconstruction with choledochocholedochostomy. (B) Biliary tract reconstruction with choledochojejunostomy, using a Roux limb.

Biliary obstruction 8 months after liver transplantation and a duct-to-duct reconstruction in a 10-year-old child. Note the ectasia of the recipient common duct (arrow). At reoperation, the graft common duct was anastomosed to a Roux limb of jejunum with a good result.

(a) Stenosis of the portal vein anastomosis (arrow) diagnosed by transhepatic portography in the same patient whose biliary system is shown in Fig. 3. (b) Operative venogram obtained through a mesenteric vein a few days later. The obstruction was complete, and the homograft portal vein was full of thrombus. (c) Patent system after resection of the sterosis, thrombectomy, and reanastomosis.

Double-drug immunosuppression with cyclosporin A and steroids. The patient (OT 198) had a hepatoma, α-1-antitrypsin deficiency, and chronic active hepatitis. The reduction of the cyclosporin A dosage after 4 days was because of the increasing azotemia. The boluses of hydrocortisone were given because of a possibly unwarranted suspicion of early rejection.

Immunosuppression with cydosporin A and steroids (plus temporary azathioprine) in a 10-year-old girl (OT 193). Note that the 5-day opening burst of prednisone therapy was scaled down because of her small size. The temporary discontinuance of cyclosporin A and replacement with azathioprine between postoperative Days 10 and 15 was because of probable cyclosporin nephrotoxicity. The patient who was of B blood type was given the liver of an A donor.

Deviation from standard steroid therapy in a patient (OT 219) whose perioperative condition was frail. The 5-day burst of postoperative steroids was begun several days postoperatively but had to be repeated when rejection supervened. Before operation, the patient had hepatorenal syndrome and encephalopathy and he had been on a ventilator for more than 1 week. Because of defective clotting, efforts to place central venous lines before starting transplantation resulted in uncontrolled hemorrhage with the loss of 20 liters of blood. The subclavian and innominant vessels were explored through cervical and thoracotomy incisions, and the bleeding was mechanically controlled before transplantation was started. The blood loss from placement of the vascular lines exceeded that incurred during transplantation. The patient survived because of prompt correction of the coagulation abnormalities. He is at home 5 months after transplantation.

Survival of three consecutive series of patients treated with orthotopic liver transplantation under conventional immunosuppression. The dashed lines in Series 2 and 3 are actuarial projections.

The life survival of adults vs. children in patients treated with conventional immunosuppression.

The actuarial survival of patients treated with cyclosporin A and low-dose steroids compared to the actual 1-year survival obtained under conventional immunosuppression by us (azathioprine) and the workers at Cambridge. The data for the Cambridge curve were obtained from published reports (53, 122).
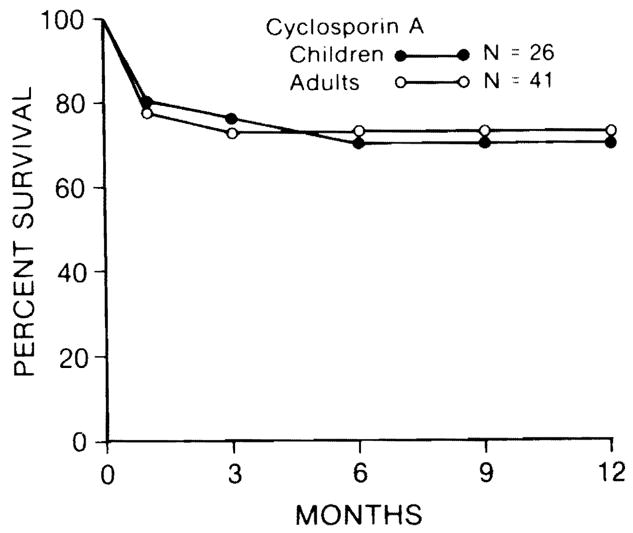
The 1-year actuarial survival of adults vs. children after liver transplantation under immunosuppression with cyclosporin A and steroids.
References
-
- Moore FD, Birtch AG, Dagher F, et al. Immunosuppression and vascular insufficiency in liver transplantation. Ann NY Acad Sci. 1964;102:729–738. - PubMed
-
- Demirleau, Noureddine, Vignes, et al. Tentative d’homogreffe hepatique (Attempted hepatic homograft) Mem Acad Chir (Paris) 1964;90:177–179. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical