

A magnetization-driven gradient echo pulse sequence for the study of myocardial perfusion
- PMID: 7476088
- PMCID: PMC2396271
- DOI: 10.1002/mrm.1910340220
A magnetization-driven gradient echo pulse sequence for the study of myocardial perfusion
Abstract
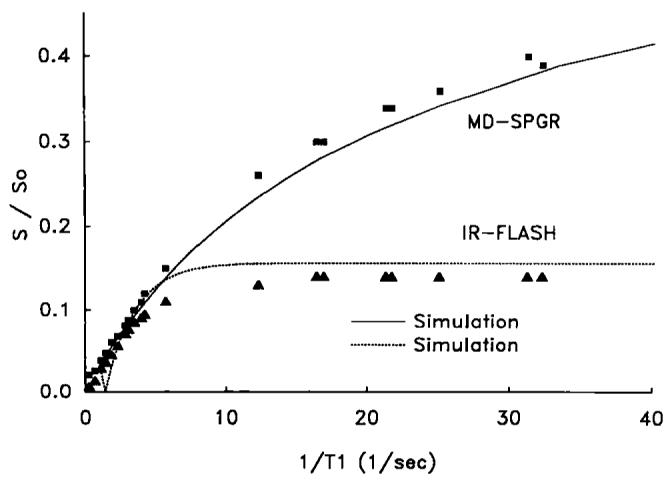
A T1-weighted imaging pulse sequence for contrast-based studies of myocardial perfusion is presented and evaluated in phantoms and in vivo. The sequence is similar to spoiled gradient-recalled echo sequences except that nonselective preparatory RF pulses drive magnetization to steady state prior to image acquisition. Steady state is thus obtained in both tissue and blood resulting in a stable, homogeneous, and dark pre-contrast baseline. Tip angles and timings are chosen so that pixel intensity approximates a linear relation to 1/T1. The dynamic range of signal response to contrast agent concentration is greater than that of an inversion-recovery fast low angle shot sequence. The sequence proposed should be useful for myocardial perfusion studies.
Figures




References
-
- Rosen BR, Belliveau JW, Vevea JM, Brady TJ. Perfusion imaging with NMR contrast agents. Magn. Reson. Med. 1990;14:249–265. - PubMed
-
- Atkinson DJ, Burstein D, Edelman RR. First-pass cardiac perfusion evaluation with ultrafast MR imaging. Radiology. 1990;174:757–762. - PubMed
-
- Wendland MF, Saeed M, Takayuki M, Derugin N, Moseley ME, Higgins CB. Echo-planar MR imaging of normal and ischemic myocardium with gadodiamide injection. Radiology. 1993;186:535–542. - PubMed
-
- Wilke N, Simm C, Zhang J, Ellerman J, Ya X, Merkle H, Path G, Ludemann H, Bache RJ, Ururbil K. Contrast-enhanced first pass myocardial perfusion imaging—correlation between myocardial blood flow in dogs at rest and during hyperemia. Magn. Reson. Med. 1993;29:485–497. - PubMed
-
- Lima JAC, Judd RM, Zerhouni EA, Schulman SP, Bazille A, Veigh McE. R., Shapiro EP, Weiss JL. Contrast enhanced ultrafast MRI demonstrates perfusion in infarcted myocardium supplied by patent coronary artery despite thallium defect. Circ. Suppl. 1993;88:1275.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
