

A new method of endoscopic variceal ligation-injection sclerotherapy (EVLIS) for gastric varices
- PMID: 7495768
- PMCID: PMC4532039
- DOI: 10.3904/kjim.1995.10.2.108
A new method of endoscopic variceal ligation-injection sclerotherapy (EVLIS) for gastric varices
Abstract
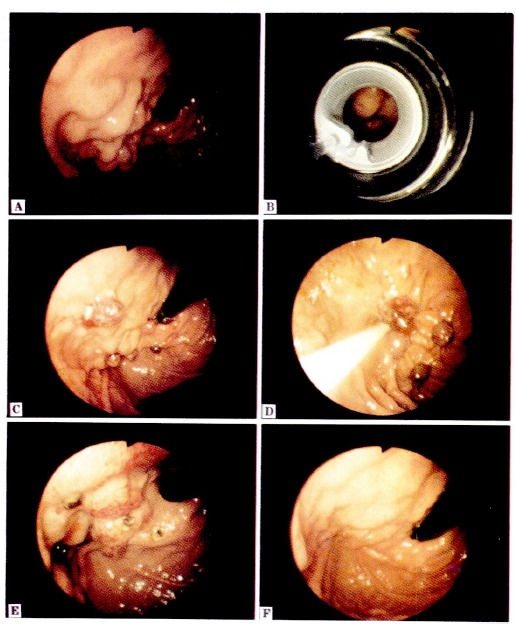
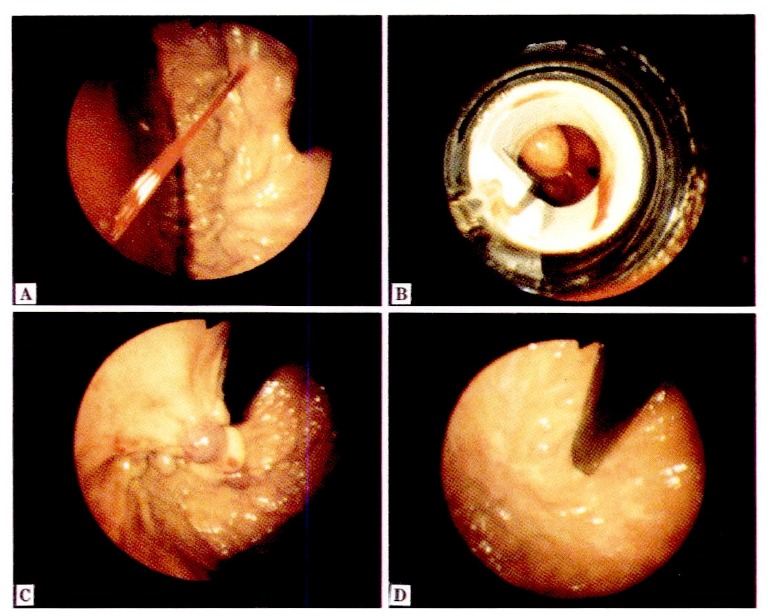
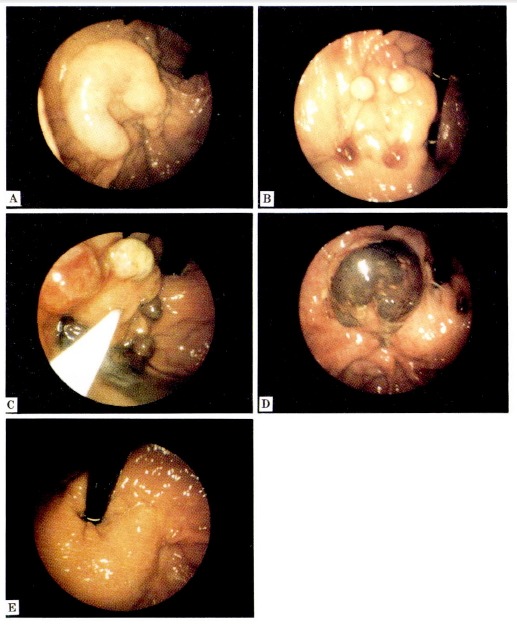
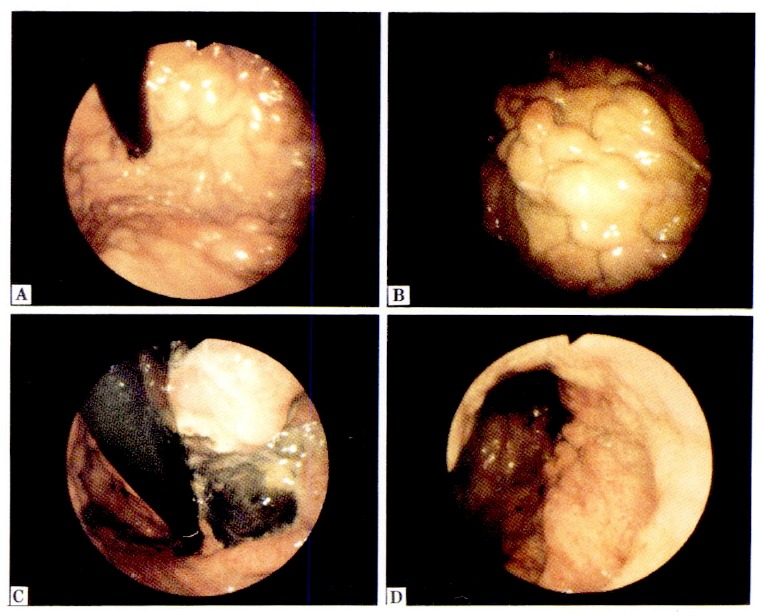
Objectives: For esophageal varices, endoscopic variceal sclerotherapy and band ligation have been effectively and frequently used, but these methods were not effective for gastric varices. In gastric varices, because of rich networks of feeding vessels and shunts that may exist in many cases, an effective therapeutic level of sclerosant is difficult to be maintained. Accordingly, we propose a new method called "Endoscopic Variceal Ligation-Injection Sclerotherapy (abbreviated EVLIS)" for gastiric varices, with focus on maintenance of the effective therapeutic level of a sclerosant by partially blocking the blood flow of gastric varices using the band ligation method. The study was undertaken prospectively to evaluate the efficacy and safety of EVLIS for the treatment of gastric varices.
Methods: EVLIS was performed in a group of 32 patients with gastric varices. Active bleeding varices were 11 and non-bleeding 21. Five cases were grade A, 12 grade B, and 14 grade C of Child's classification. Nine cases were type 1, 22 type 2, and 1 was type 3 of Hosking-Johnson's classification.
Results: The results of EVLIS were excellent, active bleeding of gastric varices in the 11 cases were successfully controlled and all the gastric varices of 32 cases including those bleeding varices were completely eradicated. The bleeding status, the Child's grade and the Hosking-Johnson's class do not appear to correlate in any way with the efficacy of this technique. No perforation or re-bleeding was observed in any of the patients until the mean 10.6 months of the follow-up period.
Conclusions: EVLIS should be considered as an effective and safe treatment for gastric varices.
Figures
References
-
- Silverstein FE, Gilbert DA, Tedesco FJ, Buenger NK, Persing J 277 members of the ASGE. The national ASGE survey on upper gastrointestinal bleeding. I. Study design and baseline data. Gastrointest Endosc. 1981;27:73. - PubMed
-
- Boyer TD. Major sequelae of cirrhosis. In: Wyngaarden JB, Smith LH, editors. Cecil textbook of medicine. 19th. Philadelphia: WB Saunders Co; 1992. p. 793.
-
- The North Italian Endoscopic club for the Study and Treatment of Esophageal Varices Prediction of the first variceal hemorrhage in patients with cirrhosis of the liver and esophageal varices. A prospective multicenter study. N Engl J Med. 1988;319:983. - PubMed
-
- Hyun JH. Endoscopic sclerotherapy of esophageal varices. J Korean Med Assoc. 1990;33(4):358.
MeSH terms
LinkOut - more resources
Full Text Sources