

Prospective cohort study of the effect of pregnancy on the progression of human immunodeficiency virus infection. The Groupe d'Epidémiologie Clinique Du SIDA en Aquitaine
- PMID: 7501333
- PMCID: PMC4749669
- DOI: 10.1016/0029-7844(95)00257-r
Prospective cohort study of the effect of pregnancy on the progression of human immunodeficiency virus infection. The Groupe d'Epidémiologie Clinique Du SIDA en Aquitaine
Abstract
Objective: To study the prognostic role of pregnancy on the progression of human immunodeficiency virus (HIV) infection.
Methods: In a prospective cohort study at the Bordeaux University Hospital, France, 57 women who completed a pregnancy during the course of their HIV infection were compared with 114 HIV-infected women who never conceived. The two groups were matched on CD4 lymphocyte count (CD4), age, and year of HIV diagnosis. The main outcome measures were death, occurrence of a first AIDS-defining event, and drop of the CD4 below 200/mm3.
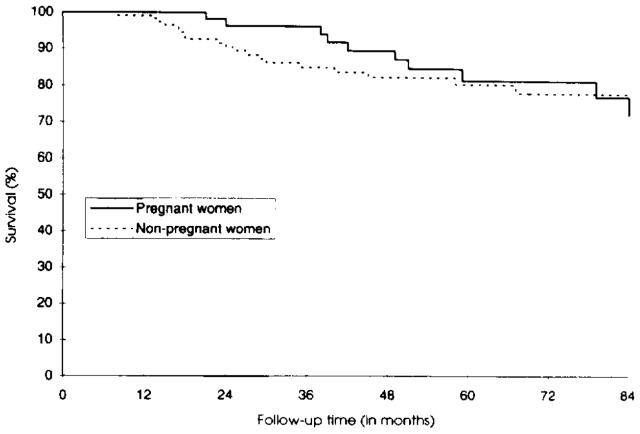
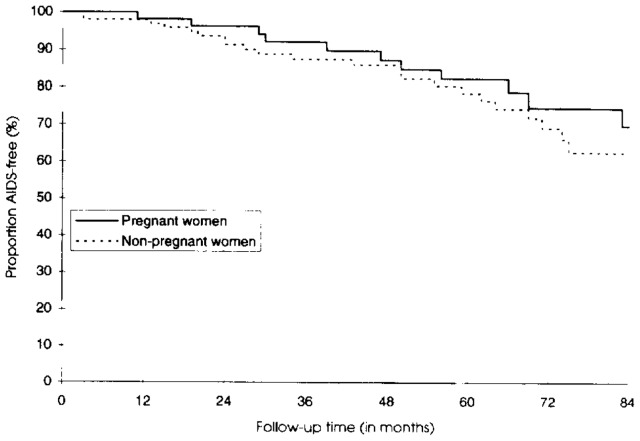
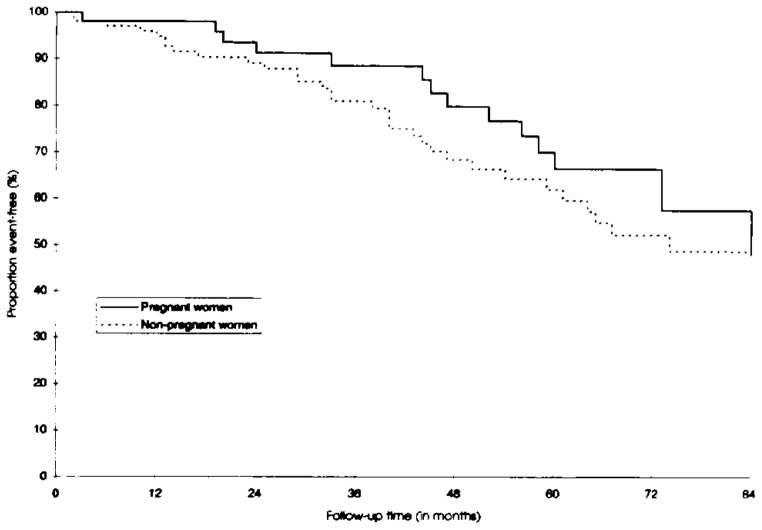
Results: The mean follow-up period in pregnant women was 61 months from HIV diagnosis (median CD4 at entry 455/mm3) and 54 months from beginning of pregnancy. Nonpregnant women were followed-up for 50 months since HIV diagnosis (median CD4 460/mm3). The proportion of asymptomatic women at entry in the study was 51 of 57 (90%) in pregnant and 87 of 114 (76%) in nonpregnant women. No significant difference was observed between the two groups with regard to the different end points studied, even after adjustment for other prognostic variables. Adjusted hazard ratios (pregnant/nonpregnant) were 0.92 for death (95% confidence interval [CI] 0.40-2.12), 1.02 for occurrence of a first AIDS-defining event (95% CI 0.48-2.18), and 1.20 for drop of the CD4 to less than 200/mm3 (95% CI 0.63-2.27).
Conclusion: In a cohort of HIV-infected women with mild to moderate immunosuppression, pregnancy did not accelerate progression to AIDS or death.
Figures
References
-
- Mandelbrot L, Henrion R. Does pregnancy accelerate disease progression in HIV-infected women? In: Johnson MA, Johstone FD, editors. HIV infection in women. Edinburgh: Churchill Livingstone; 1993. pp. 157–71.
-
- Scott GB, Fischl MA, Klimas N, Fletcher MA, Dickinson GM. Mothers of infants with the acquired immunodeficiency syndrome. JAMA. 1985;253:363–6. - PubMed
-
- Minkoff H, Nanda D, Menez R, Fikrig S. Pregnancies resulting in infants with acquired immunodeficiency syndrome or AIDS-related complex: Follow-up of mothers, children, and subsequently born siblings. Obstet Gynecol. 1987;69:288–91. - PubMed
-
- Lindgren S, Anzen B, Bohlin AB, Lidman K. HIV and childbearing: Clinical outcome and aspects of mother to infant transmission. AIDS. 1991;5:1111–6. - PubMed
-
- Schafer A. The effects of pregnancy on the natural evolution of HIV infection. The experience of Berlin. In: Berrebi, editor. HIV infection in mother and child. Paris: Privat; 1988. pp. 127–47.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
