

Three years clinical experience with intestinal transplantation
- PMID: 7522850
- PMCID: PMC2677020
Three years clinical experience with intestinal transplantation
Abstract
Background: After the successful evolution of hepatic transplantation during the last decade, small bowel and multivisceral transplantation remains the sole elusive achievement for the next era of transplant surgeons. Until recently, and for the last thirty years, the results of the sporadic attempts of intestinal transplantation worldwide were discouraging because of unsatisfactory graft and patient survival. The experimental and clinical demonstration of the superior therapeutic efficacy of FK 506, a new immunosuppressive drug, ushered in the current era of small bowel and multivisceral transplantation with initial promising results.
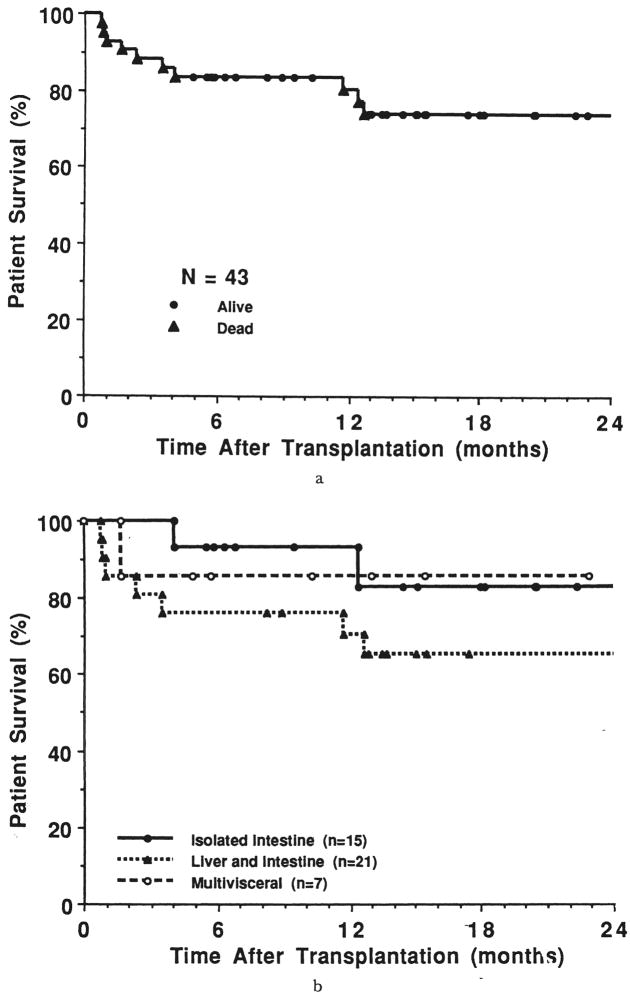
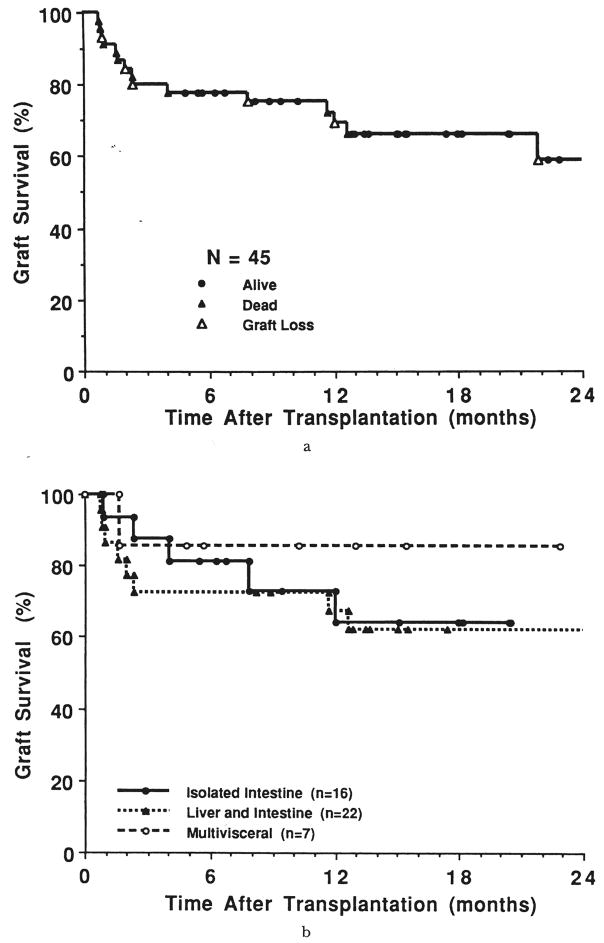
Study design: Forty-three consecutive patients with short bowel syndrome, intestinal insufficiency, or malignant tumors with or without associated liver disease, were given intestinal (n = 15), hepatic and intestinal (n = 21), or multivisceral allografts that contained four or more organs (n = 7). Treatment was with FK 506 based immunosuppression. The ascending and right transverse colon were included with the small intestine in 13 of the 43 grafts, almost evenly distributed between the three groups.
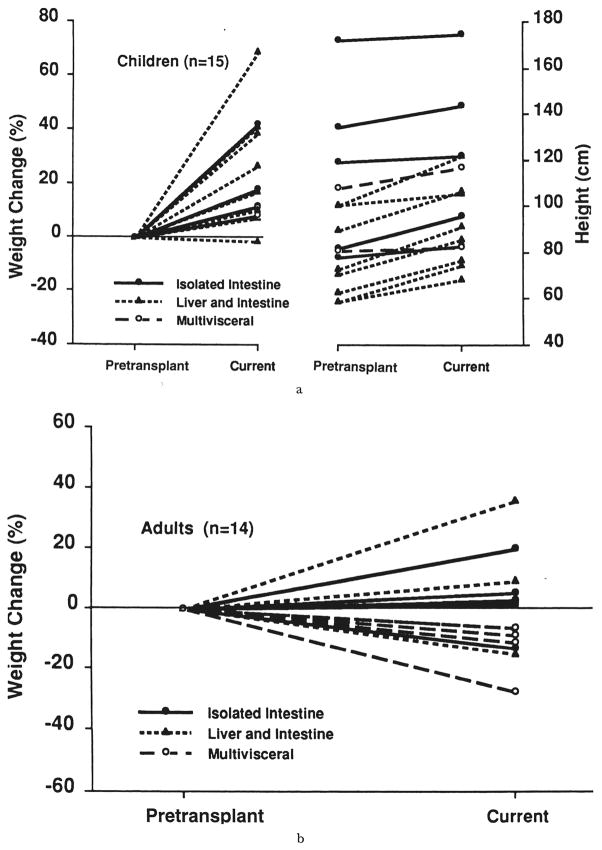
Results: After six to 39 months, 30 of the 43 patients are alive, 29 bearing grafts. The most rapid convalescence and resumption of diet, as well as the highest three month patient survival (100 percent) and graft survival (88 percent) were with the isolated intestinal procedure. However, this advantage was slowly eroded during the first two postoperative years, in part because the isolated intestine was more prone to rejection. By the end of this time, the best survival rate (86 percent) was with the multivisceral procedure. With all three operations, most of the patients were able to resume diet and discontinue parenteral alimentation, and in the best instances, the quality of life approached normal. However, the surveillance and intensity of care required for these patients for the first year, and in most instances thereafter, was very high, being far more than required for patients having transplants of the liver, kidney or heart.
Conclusions: Although intestinal transplantation has gone through the feasibility phase, strategies will be required to increase its practicality. One possibility is to combine intestinal transplantation with contemporaneous autologous bone marrow transplantation.
Figures




References
-
- Grant D, Wall W, Mimeault R, et al. Successful small-bowel/liver transplantation. Lancet. 1990;335:181–184. - PubMed
-
- Deltz E, Schroeder P, Gebhardt H, et al. Successful clinical small bowel transplantation: report of a case. Clin Transpl. 1989;3:89–91.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources