

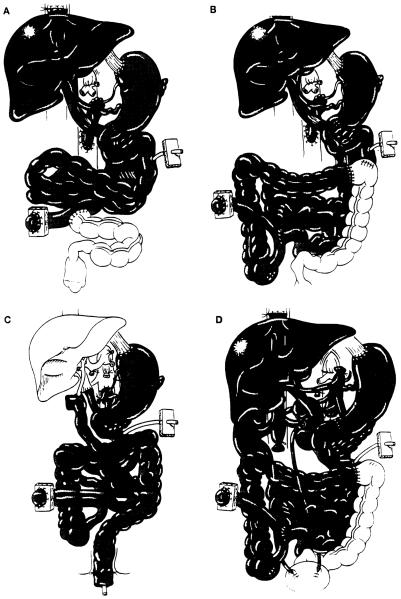
Abdominal multivisceral transplantation
- PMID: 7530873
- PMCID: PMC2953264
- DOI: 10.1097/00007890-199501270-00015
Abdominal multivisceral transplantation
Abstract
Under FK506-based immunosuppression, 13 abdominal multivisceral transplantations were performed in 6 children and 7 adults. Of the 13 recipients, 7 (53.8%) are alive and well with functioning grafts after 9 to 31 months. Six recipients died: three from PTLD, one from rejection, one from sepsis, and one from respiratory failure. In addition to rejection, postoperative complications occurring in more than isolated cases included PTLD (n = 6), abdominal abscess formation (n = 5), pancreatitis (n = 3), and ampullary dysfunction (n = 2). In addition, infection by enteric microorganisms was common during the early postoperative period. Currently, all 7 survivors are on an oral diet and have normal liver function. Two recipients (one insulin-dependent) require antidiabetes treatment, in one case following distal pancreatectomy and in the other after two episodes of pancreatic rejection. Thus, abdominal multivisceral transplantation is a difficult but feasible operation that demands complex and prolonged posttransplantation management. It is not yet ready for application and awaits a better strategy of immune modulation.
Figures
References
-
- Williams JW, Sankary HN, Foster PF, Lowe J, Goldman GM. Splanchnic transplantation: an approach to the infant dependent on parenteral nutrition who develops irreversible liver disease. JAMA. 1989;261:1458. - PubMed
-
- Margreiter R, Konigsrainer A, Schmid T, et al. Successful multivisceral transplantation. Transplant Proc. 1992;24:1226. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources