

Variable chimerism, graft-versus-host disease, and tolerance after different kinds of cell and whole organ transplantation from Lewis to brown Norway rats
- PMID: 7624958
- PMCID: PMC3003921
- DOI: 10.1097/00007890-199507000-00009
Variable chimerism, graft-versus-host disease, and tolerance after different kinds of cell and whole organ transplantation from Lewis to brown Norway rats
Abstract
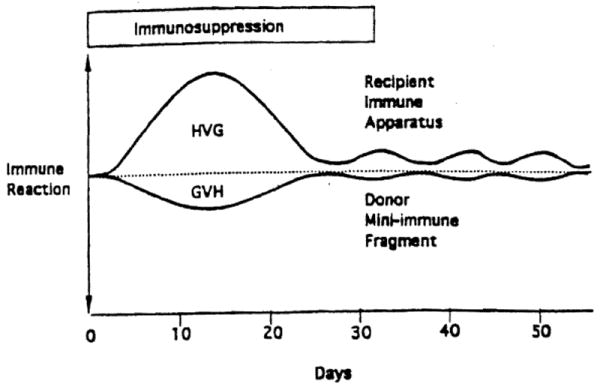
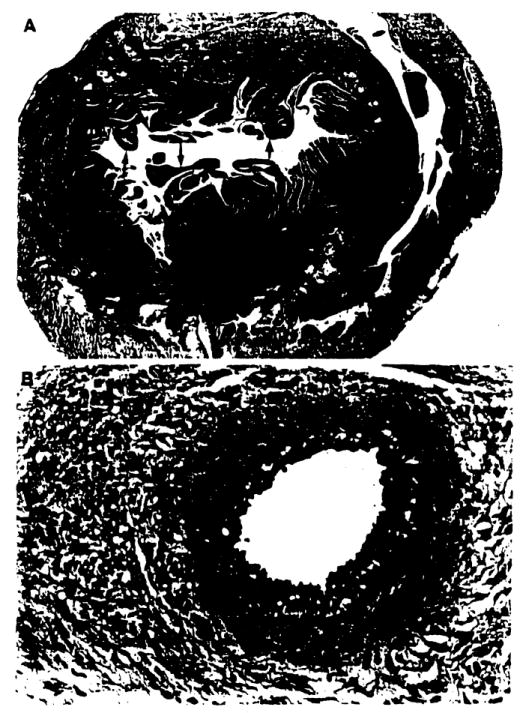
The bidirectional paradigm of tolerance involving reciprocal host vs. graft and graft vs. host reactions was examined after Lewis (LEW)-->Brown Norway (BN) transplantation of different whole organs (liver, intestine, heart, and kidney) or of 2.5 x 10(8) LEW leukocytes obtained from bone marrow, spleen, lymph nodes, and thymus. The experiments were performed without immunosuppression or under 14 daily doses of postoperative tacrolimus, which were continued in weekly doses to 100 days in a "continuous treatment" subgroup, and to 27 days in a short treatment group. Without immunosuppression, all organs and cell suspensions failed to engraft or were acutely rejected. GVHD (usually fatal) was always caused when either the long or short treatment was used for recipients of intestinal grafts and cell suspensions of spleen and lymph nodes. In contrast, both immunosuppressive protocols allowed engraftment of bone marrow cells, liver, heart, and kidney without clinical GVHD, whereas thymus cell suspensions and small doses of whole blood neither engrafted nor caused GVHD. At 100 days, now drug-free for 73 days, the liver, bone marrow, and heart recipients were tolerant in that they accepted all challenge LEW heart and/or liver grafts for 100 more days despite in vitro evidence of donor-specific reactivity (split tolerance). At 200 days, histopathologic studies of the challenge livers were normal no matter what the priming graft. However, the still-beating challenge hearts had a spectrum from normal to severe chronic rejection that defined the tolerogenicity of the original primary grafts: liver best-->bone marrow next-->heart least. Both the GVHD propensity and tolerogenicity in these experiments were closely associated with recipient tissue chimerism 30 and 100 days after the experiments began. The tissue chimerism was invariably multilineage, but the GVHD outcome was associated with T cell over-representation. These observations provide guidelines that should be considered in devising leukocyte augmentation protocols for human whole organ recipients. The results are discussed in relation to the historical tolerance studies of Billingham, Brent, and Medawar; Good; Monaco; and Calne.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources