

Evaluation of sequential serum interleukin-6 levels in liver allograft recipients
- PMID: 8165699
- PMCID: PMC3022505
- DOI: 10.1097/00007890-199404150-00009
Evaluation of sequential serum interleukin-6 levels in liver allograft recipients
Abstract
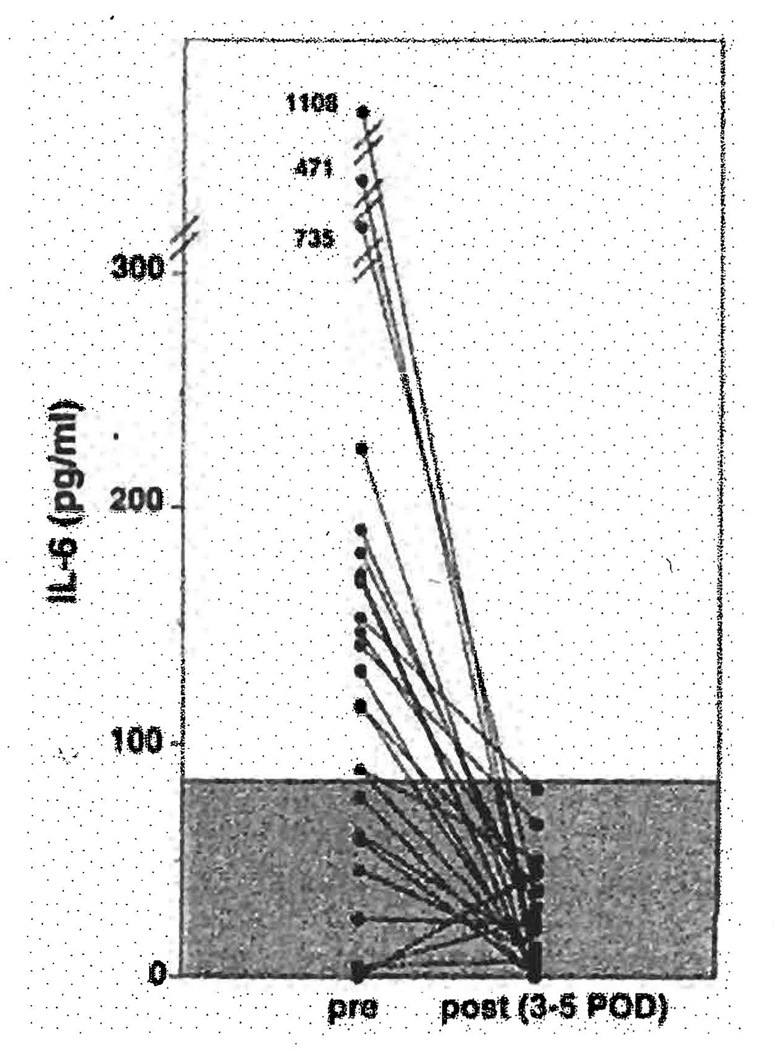
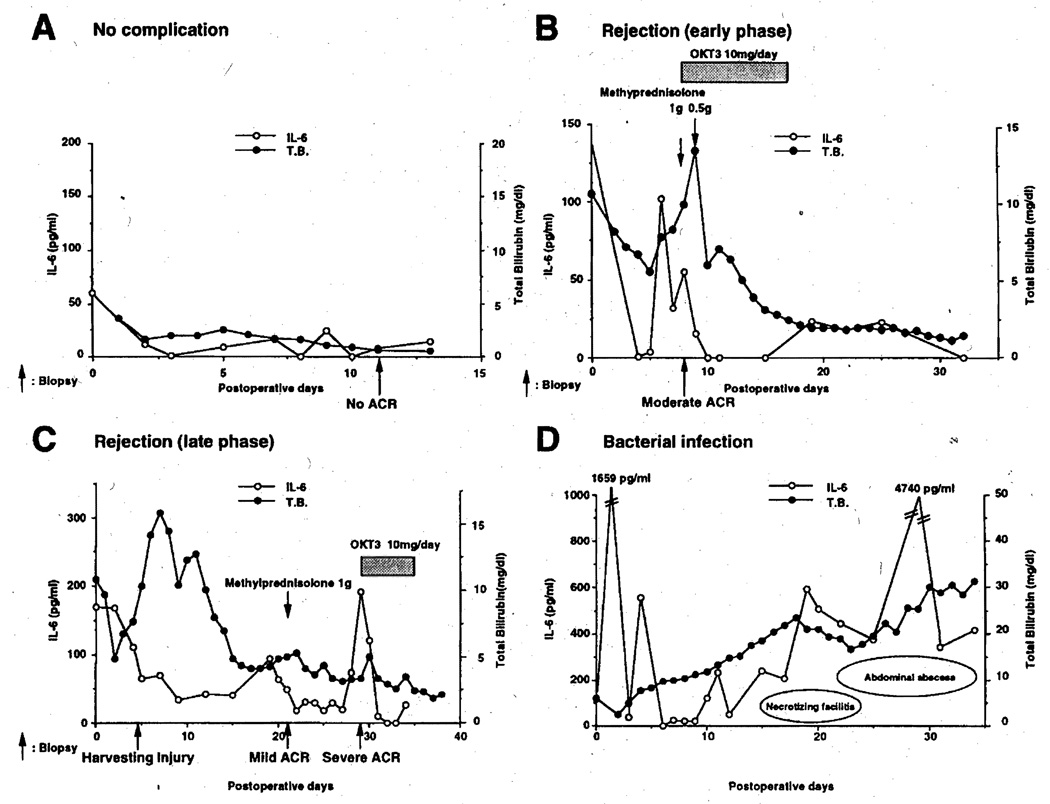
Control serum levels of IL-6 measured by ELISA in 30 healthy blood donors or volunteers were 18 +/- 34 pg/ml (mean +/- SD). Pretransplant serum levels of IL-6 in 169 adult candidates for liver transplantation were significantly higher than control in those with fulminant hepatitis (203 +/- 232 pg/ml), alcoholic cirrhosis (116 +/- 257 pg/ml), and hepatocellular carcinoma (82 +/- 105 pg/ml). With these data as background, plasma or serum levels of IL-6 were monitored in 24 adult patients after first OLT and correlated with the clinical courses and the histopathological diagnosis of rejection. Serum or plasma levels of IL-6 decreased after transplantation regardless of pretransplant value. Four patients with infection subsequently developed continuously high IL-6 values. In the 20 of 24 patients who did not have infection, significantly higher levels of IL-6 were consistently found 0-4 days before histopathological diagnosis of rejection (131 +/- 78 pg/ml) compared with significantly lower values in patients without rejection episodes (40 +/- 21 pg/ml). The elevations of IL-6 were spike shaped, did not correlate well with the histopathological grades of rejection, and were highly responsive to augmented immunosuppression. These 20 cases were classified as: group 1, no spikes of IL-6 after liver transplantation; group 2, single spike of IL-6 after liver transplantation; and group 3, multiple spikes of IL-6 after liver transplantation. The combined early and late graft loss of each group was 0% (group 1), 25% (group 2), and 67% (group 3). We conclude that daily monitored serum or plasma IL-6 levels can be a good premonitor of liver allograft rejection and also a useful predictor of long-term graft outcome.
Figures
References
-
- Kishimoto T. The biology of interleukin-6. Blood. 1989;74:1. - PubMed
-
- Van Snick J. Interleukin-G: an overview. Annu Rev Immunol. 1990;8:253. - PubMed
-
- Fey GH, Gauldie J. The acute phase response of the liver inflammation. In: Popper H, Schaffner F, editors. Progress in liver disease. Vol 9. Philadelphia: WB Saunders; 1990. p. 89. - PubMed
-
- Castell JV, Geiger T, Gross V, et al. Plasma clearance, organ distribution and target cells of interleukin 6/hepatocyte-stimulating factor in the rat. Eur J Biochem. 1988;177:357. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical