

Prospective comparative study of ability of MR imaging and other imaging modalities to localize tumors in patients with Zollinger-Ellison syndrome
- PMID: 8325191
- PMCID: PMC6721850
- DOI: 10.1007/BF01296084
Prospective comparative study of ability of MR imaging and other imaging modalities to localize tumors in patients with Zollinger-Ellison syndrome
Abstract
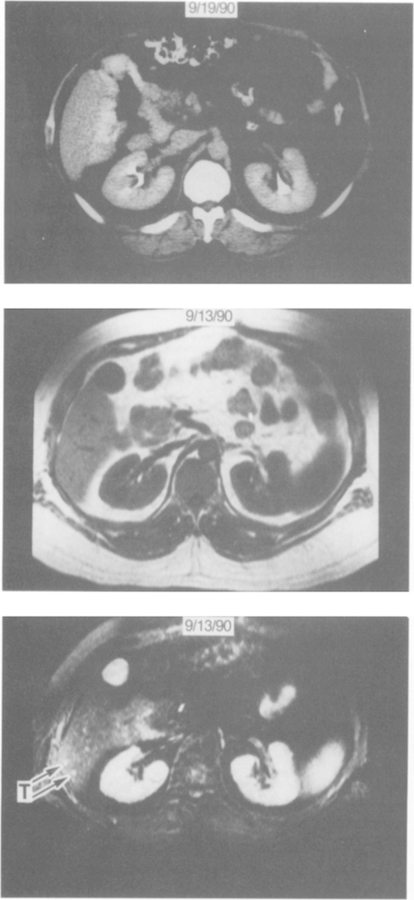
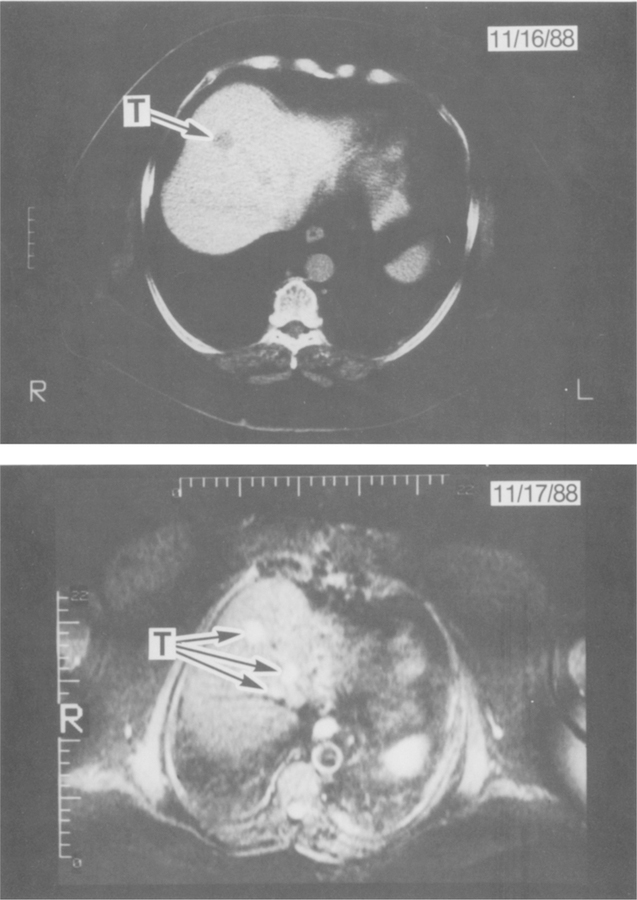
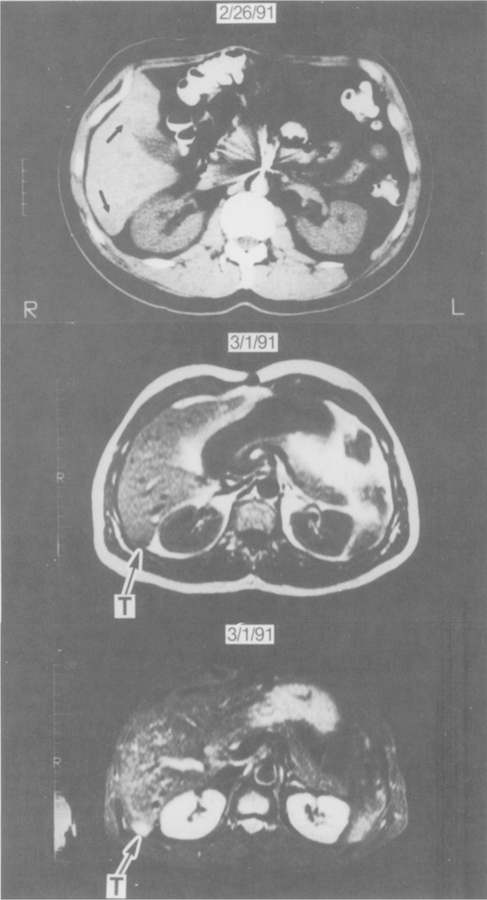
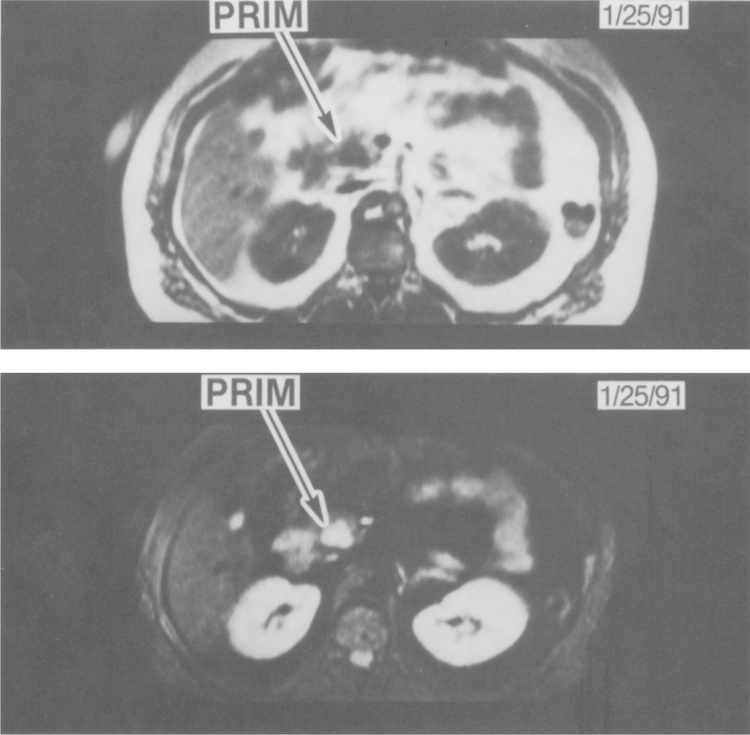
The role of magnetic resonance (MR) imaging in patients with pancreatic endocrine tumors such as Zollinger-Ellison syndrome (ZES) is controversial. In the present study we have examined the ability of current MR imaging compared with other imaging modalities, to localize gastrinomas in 43 patients with ZES. All results were subsequently assessed at exploratory laparotomy (N = 34) or by liver biopsy (N = 9). For the 18 patients with metastatic gastrinoma in the liver, MR imaging had a sensitivity of 83%, ultrasound 50%, CT 56%, and angiography 61%. The combination of MR imaging, ultrasound, and CT were the same as MR imaging alone. For MR imaging, both T1 and STIR sequences had equal sensitivity, although tumors were more easily seen with STIR sequences. Specificity of MR imaging was slightly lower (88%) than the other modalities (96-100%) because MR imaging incorrectly identified small hemangiomas as possible tumors in four patients. MR imaging was better than CT in identifying metastatic lesions in the liver. For the localization of primary gastrinoma, assessed in 32 patients, MR imaging had a sensitivity of 25%, ultrasound 19%, CT 28%, all three together 38%, and angiography 59%. Localization of metastatic gastrinoma in the liver or primary gastrinomas in 16 patients was assessed before and after gadolinium-DTPA (0.1 mmol/kg). The sensitivity and specificity of MR imaging was unchanged but bolus injection and rapid MR acquisition techniques were not used. These results indicate that recent advances in MR imaging have greatly improved its sensitivity for the detection and assessment of the extent of metastatic gastrinoma. MR imaging is now the imaging study of choice to assess metastatic pancreatic endocrine tumors in the liver. In contrast, the detection of primary tumors by MR imaging has not improved; therefore, angiography remains the study of choice.
Figures
References
-
- Jensen RT, Norton JA: Endocrine neoplasms. In Textbook of Gastroenterology Yamada T (ed). Philadelphia, JB: Lippincott, 1991, pp 1912–1937
-
- Norton JA, Doppman JL, Jensen RT: Cancer of the endocrine system. In Principles and Practice of Oncology, 3rd ed. DeVita VT, Helman S, Rosenberg SA, (eds). Philadelphia, JB: Lippincott, 1989, pp 1269–1344
-
- Jensen RT, Maton PN: Zollinger-Ellison syndrome. In The Stomach Gustavsson S, Kumar D, Graham DY (eds). London, Churchill-Livingstone, 1991, pp 341–374
-
- Saeed ZA, Doppman JL, Norton J, Maton PN, Gardner JD, Jensen RT: Gastrinoma localization in Zollinger-Ellison syndrome. Intern Med Spec 9:79–99, 1988
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical