

Treatment of narcolepsy with methamphetamine
- PMID: 8341891
- PMCID: PMC2267865
Treatment of narcolepsy with methamphetamine
Abstract
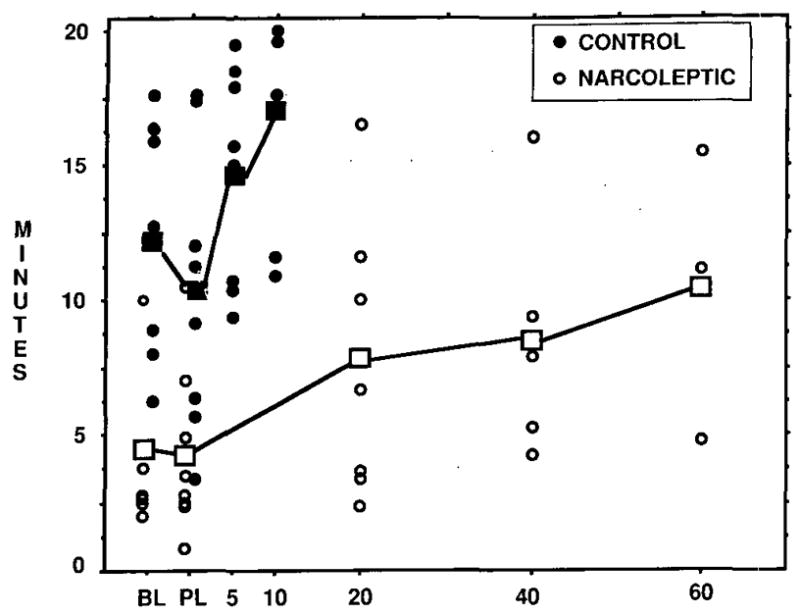
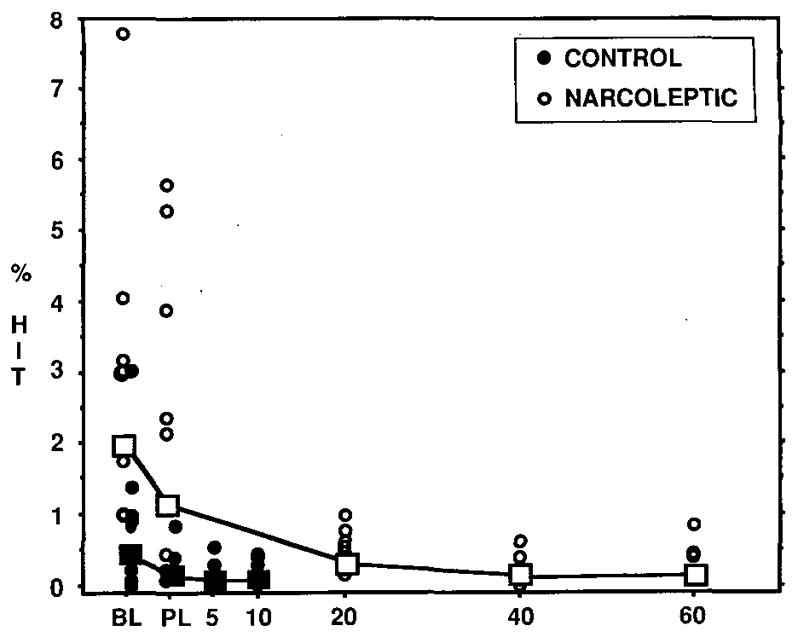
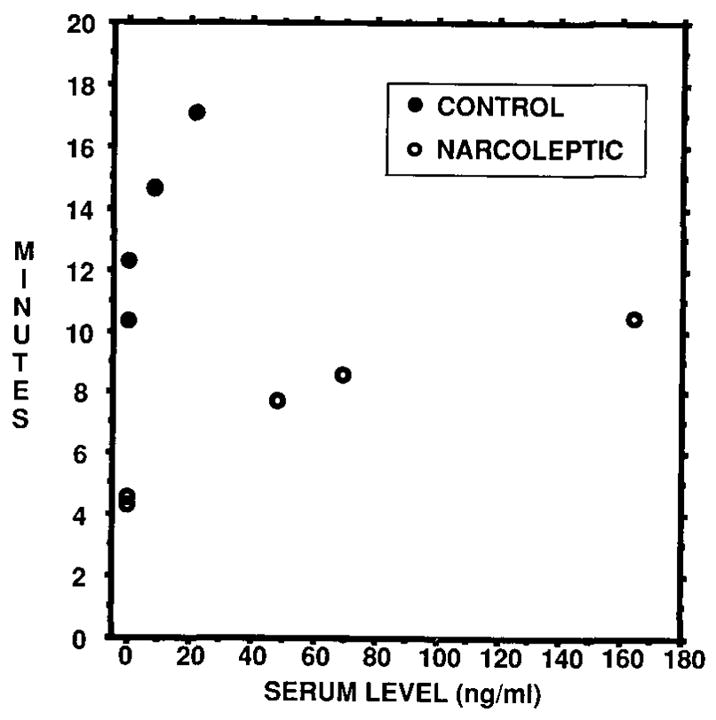
Eight pairs of subjects (each consisting of a narcoleptic and a control matched on the basis of age, sex, educational background and job) were evaluated under the following double-blind, randomized treatment conditions: baseline, placebo, low dose and high dose methamphetamine. Subjects were drug-free for 2 weeks prior to beginning the protocol. Methamphetamine was the only drug taken during the protocol and was given in a single morning dose of 0, 20 or 40-60 mg to narcoleptics and 0, 5 or 10 mg to controls. The protocol was 28 days long, with each of the four treatment conditions lasting 4 days followed by 3 days of washout. Nighttime polysomnography and daytime testing were done during the last 24 hours of each treatment condition. Daytime sleep tendency was assessed with the multiple sleep latency test (MSLT). Daytime performance was assessed with performance tests including a simple, computer-based driving task. Narcoleptics' mean MSLT sleep latency increased from 4.3 minutes on placebo to 9.3 minutes on high dose, compared with an increase from 10.4 to 17.1 minutes for controls. Narcoleptics' error rate on the driving task decreased from 2.53% on placebo to 0.33% on high dose, compared with a decrease from 0.22% to 0.16% for controls. The effects of methamphetamine on nocturnal sleep were generally dose-dependent and affected sleep continuity and rapid eye movement (REM) sleep. Elimination half life was estimated to be between 15.9 and 22.0 hours. Mild side effects emerged in a dose-dependent fashion and most often involved the central nervous system and gastrointestinal tract. We concluded that methamphetamine caused a dose-dependent decrease in daytime sleep tendency and improvement in performance in both narcoleptics and controls. Methamphetamine at doses of 40-60 mg allowed narcoleptics to function at levels comparable to those of unmedicated controls.
Figures
References
-
- Kurland LT, Mulder DW, Westlund KB. Multiple sclerosis and amyotrophic lateral sclerosis: etiologic significance of recent epidemiologic and genetic studies. New Engl J Med. 1955;252:649–53. - PubMed
-
- Kurland LT, Mulder DW, Westlund KB. Multiple sclerosis and amyotrophic lateral sclerosis (concluded): etiologic significance of recent epidemiologic and genetic studies. New Engl J Med. 1955;252:697–702. - PubMed
-
- Dement W, Zarcone V, Varner V, et al. The prevalence of narcolepsy. Sleep Res. 1972;1:147.
-
- Dement W, Carskadon M, Ley R. The prevalence of narcolepsy II. Sleep Res. 1973;2:147.
-
- Fruhstorfer B, Mignot E, Bowersox S, Nishino S, Dement WC, Guilleminault C. Canine narcolepsy is associated with an elevated number of alpha 2-receptors in the locus coeruleus. Brain Research. 1989;500:209–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical