

High-inflation pressure and positive end-expiratory pressure. Injurious to the lung? Yes
- PMID: 8839594
- PMCID: PMC9585904
- DOI: 10.1016/s0749-0704(05)70266-9
High-inflation pressure and positive end-expiratory pressure. Injurious to the lung? Yes
Abstract
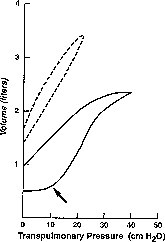
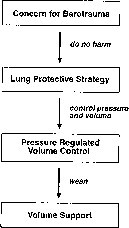
There is a growing body of evidence suggesting that high levels of inflation pressure and high levels of PEEP may be injurious to lung tissue and other organ systems. Limiting peak alveolar pressures below 35 cm H2O may help in avoiding these injuries. The findings have led to the development of a lung-protective strategy that is based on physiologic parameters. This strategy, often using permissive hypercapnia and pressure-limited modes of ventilation, may gain widespread use in the near future. If this strategy reduces barotrauma, a reduction in the length of time on mechanical ventilation and mortality rates can be anticipated. At our center we routinely initiate mechanical ventilation in patients with acute lung injury, using tidal volumes of approximately 6 mL/kg. This may be decreased further if peak alveolar pressures exceed 30 to 35 cm H2O. PEEP is added to maximize alveolar recruitment and oxygenation. Optimal PEEP is located at the inflection point of the respiratory compliance curve. Usually a PEEP of 8 to 12 cm H2O is sufficient. Although we usually initiate mechanical ventilation with a volume-cycled mode, we are not hesitant to switch rapidly to a pressure-limited mode if results are unsatisfactory. We believe that more attention to the potential harmful effects of pressure and volume on lung architecture may result in further improvement of survival in patients with acute respiratory failure.
Figures
Similar articles
-
Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome.N Engl J Med. 1998 Feb 5;338(6):347-54. doi: 10.1056/NEJM199802053380602. N Engl J Med. 1998. PMID: 9449727 Clinical Trial.
-
High-inflation pressure and positive end-expiratory pressure. Injurious to the lung? No.Crit Care Clin. 1996 Jul;12(3):603-25. doi: 10.1016/s0749-0704(05)70265-7. Crit Care Clin. 1996. PMID: 8839593 Review.
-
Tidal ventilation at low airway pressures can augment lung injury.Am J Respir Crit Care Med. 1994 May;149(5):1327-34. doi: 10.1164/ajrccm.149.5.8173774. Am J Respir Crit Care Med. 1994. PMID: 8173774
-
Rationale, study design, and analysis plan of the Alveolar Recruitment for ARDS Trial (ART): study protocol for a randomized controlled trial.Trials. 2012 Aug 28;13:153. doi: 10.1186/1745-6215-13-153. Trials. 2012. PMID: 22929542 Free PMC article. Clinical Trial.
-
Lung recruitment maneuvers in acute respiratory distress syndrome and facilitating resolution.Crit Care Med. 2003 Apr;31(4 Suppl):S265-71. doi: 10.1097/01.CCM.0000057902.29449.29. Crit Care Med. 2003. PMID: 12682451 Review.
Cited by
-
Safety of Small-Diameter Endotracheal Tubes in Microlaryngeal Surgery.Laryngoscope. 2025 Apr;135(4):1451-1454. doi: 10.1002/lary.31865. Epub 2024 Oct 31. Laryngoscope. 2025. PMID: 39479955
References
-
- Cullen D.J., Caldena D.L. The incidence of ventilator-induced pulmonary barotrauma in critically ill patients. Anesthesiology. 1979;50:185–190. - PubMed
-
- DeRusso S.M., Nelson L.D., Safcsak K., et al. Survival in patients with severe adult respiratory distress syndrome treated with high-level, positive end expiratory pressure. Crit Care Med. 1995;23:1485–1496. - PubMed
-
- Dreyfuss D., Soler P., Saumon G. Mechanical ventilation-induced pulmonary edema: Interaction with previous lung alterations. Am J Respir Crit Care Med. 1995;151:1568–1575. - PubMed
-
- Gattinoni L., Presenti A. ARDS: The non-homogeneous lung: Facts and hypothesis. Critical Care Diagnosis. 1987;6:1–4.
-
- Gattinoni L., Presenti A., Bombino M. Relationships between lung computed tomographic density, gas exchange, and PEEP in acute respiratory failure. Anesthesiology. 1988;69:824–832. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
