

Parathyroid hormone-related peptide (PTHrP) regulates fetal-placental calcium transport through a receptor distinct from the PTH/PTHrP receptor
- PMID: 8986793
- PMCID: PMC26386
- DOI: 10.1073/pnas.93.26.15233
Parathyroid hormone-related peptide (PTHrP) regulates fetal-placental calcium transport through a receptor distinct from the PTH/PTHrP receptor
Abstract
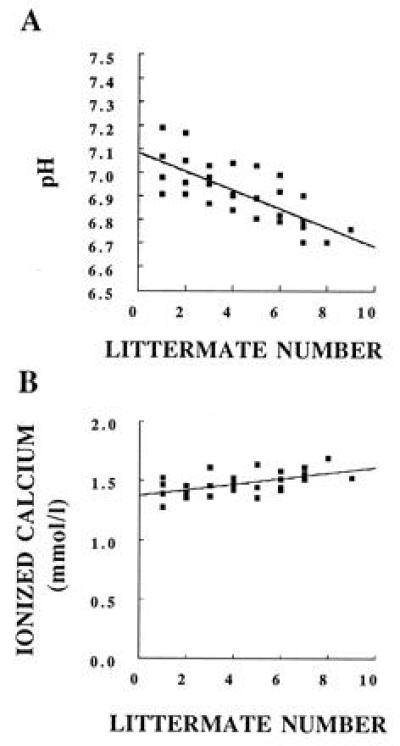
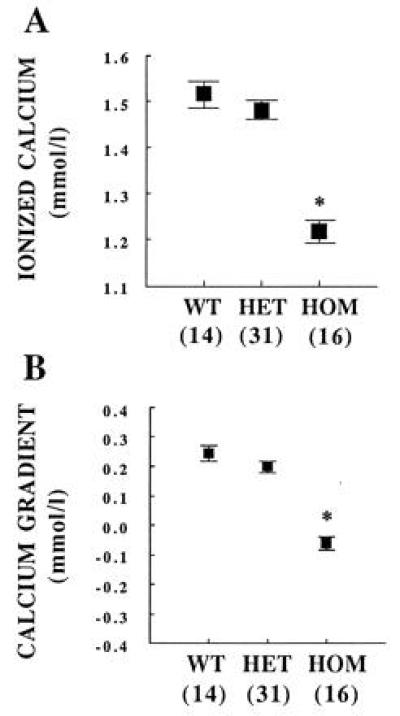
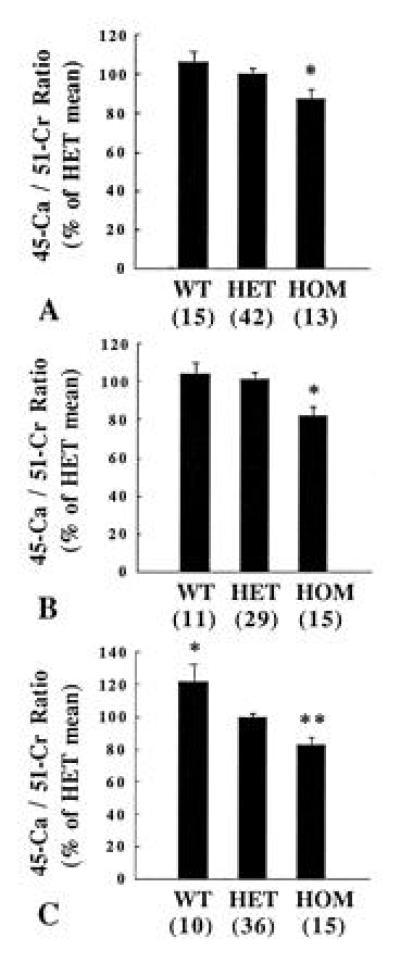
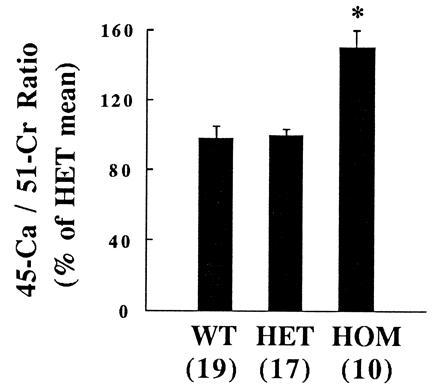
To determine the role of PTHrP in fetal calcium metabolism, blood calcium was measured in mice homozygous (HOM) for deletion of the PTHrP gene. On day 18.5 of gestation, ionized calcium and the maternal-fetal calcium gradient were significantly reduced in HOM PTHrP-ablated fetuses compared with that of their littermates. To assess the placental contribution to the effect of PTHrP, 45Ca and 51Cr-EDTA (as a blood diffusional marker) were administered by intracardiac injection to pregnant, heterozygous dams on day 17.5 of gestation. Five minutes after the injection, whole fetal 45Ca accumulation was significantly decreased in HOM PTHrP-ablated fetuses compared with that of their littermates. Next, two fetuses from each litter were injected in utero with fragments of PTHrP, PTH, or diluent 1 h before administering 45Ca and 51Cr to the dam. PTHrP-(1-86) and PTHrP-(67-86) significantly increased relative 45Ca accumulation in HOM PTHrP-ablated fetuses, but PTHrP-(1-34), PTH-(1-84), and the diluent had no effect. Finally, similar studies were performed on fetal mice that lacked the PTH/PTHrP receptor gene. Ionized calcium was significantly reduced in HOM PTH/PTHrP receptor-ablated fetuses. However, 5 min after maternal injection of 45Ca and 51Cr, relative accumulation of 45Ca was significantly increased in these fetuses. It was concluded that PTHrP is an important regulator of fetal blood calcium and placental calcium transport. In addition, the bioactivity of PTHrP for placental calcium transport is specified by a mid-molecular region that does not use the PTH/PTHrP receptor.
Figures
References
-
- Fisher G J, Kelley L K, Smith C H. Am J Physiol. 1987;252:C38–C46. - PubMed
-
- Borke J L, Caride A, Verma A K, Kelley L K, Smith C H, Penniston J T, Kumar R. Am J Physiol. 1989;257:C341–C346. - PubMed
-
- Garel J M, Barlet J P. Pediatr Res. 1976;10:749–754. - PubMed
-
- Hollis B W, Pittard W B. J Clin Endocrinol Metab. 1984;59:652–657. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
