

Role of NMDA and non-NMDA ionotropic glutamate receptors in traumatic spinal cord axonal injury
- PMID: 8994060
- PMCID: PMC6573164
- DOI: 10.1523/JNEUROSCI.17-03-01055.1997
Role of NMDA and non-NMDA ionotropic glutamate receptors in traumatic spinal cord axonal injury
Abstract
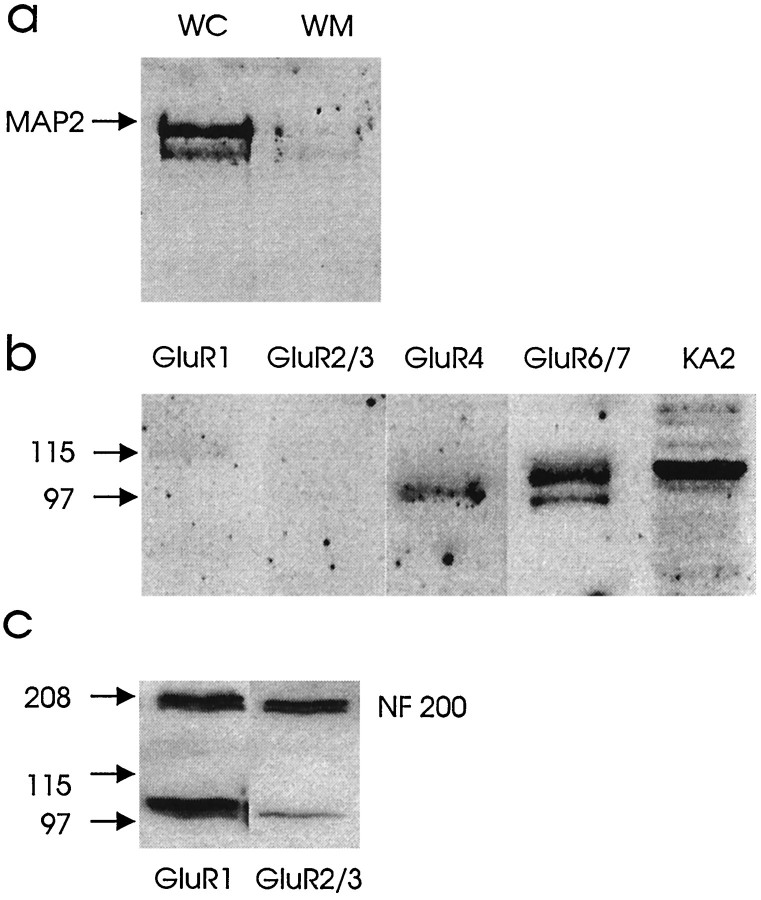
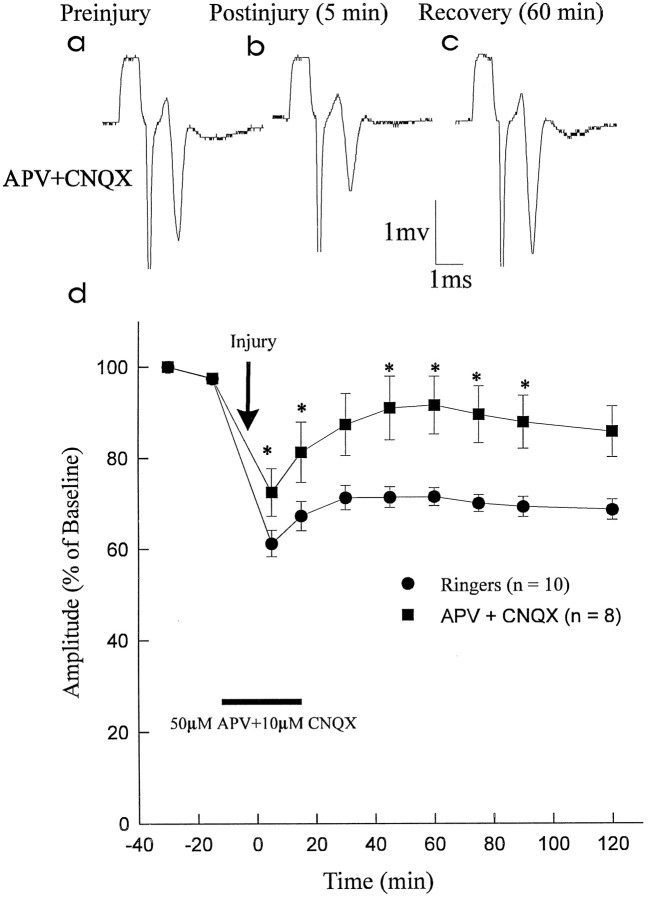
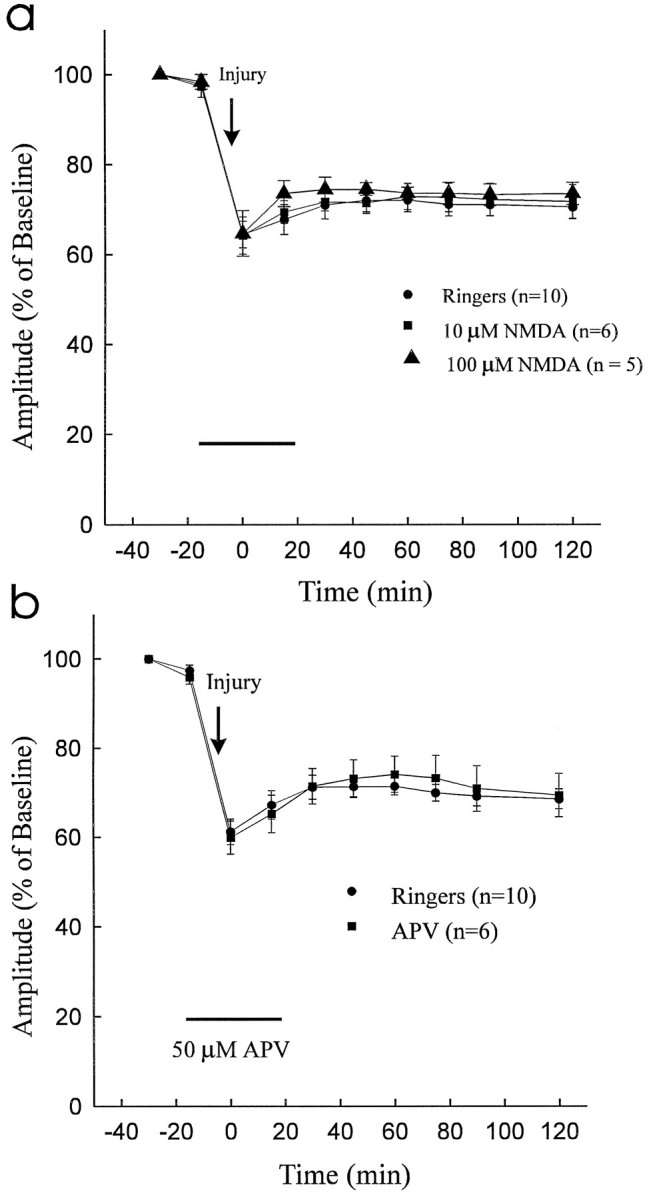
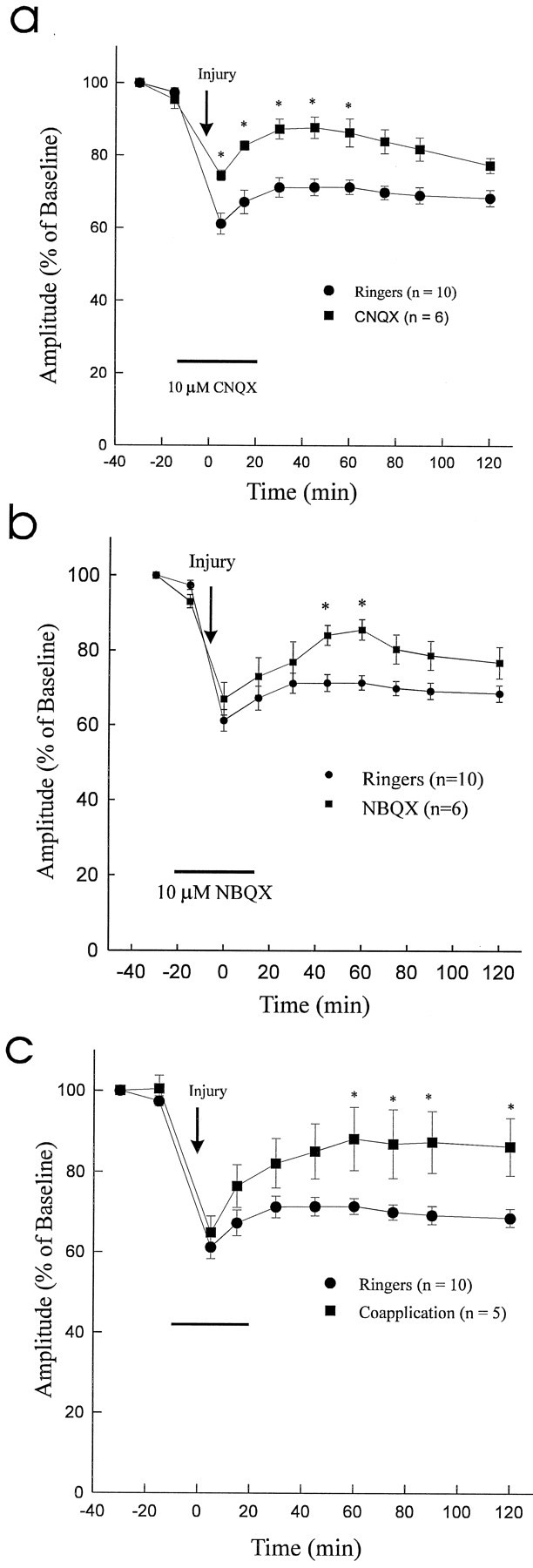
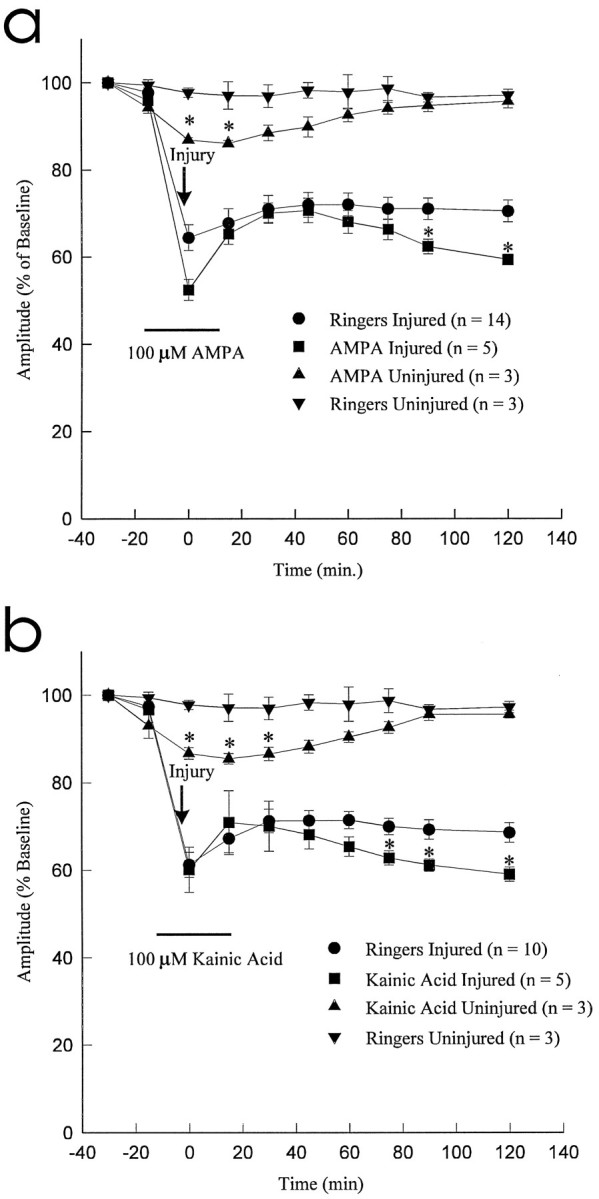
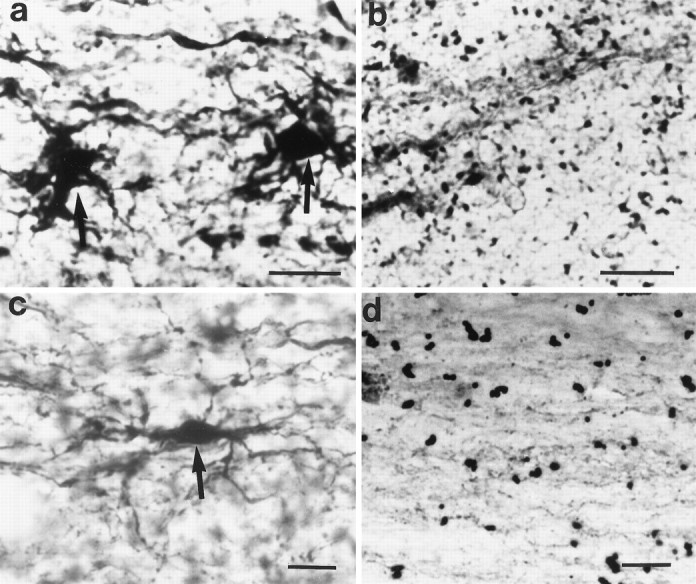
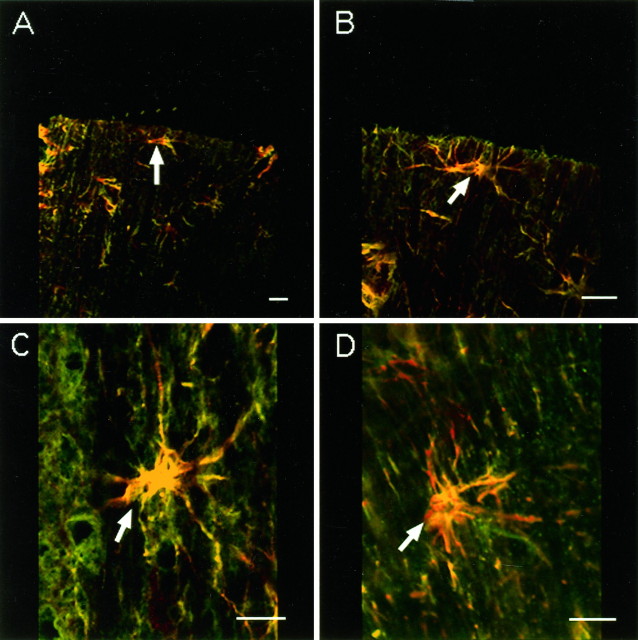
We examined the role of glutamatergic mechanisms in acute injury to rat spinal cord white matter. Compound action potentials (CAPs) were recorded from isolated dorsal column segments in vitro. Under control conditions (Ringer's solution), the CAPs decreased to 71.4 +/- 2.0% of preinjury values after compression injury with a clip exerting a closing force of 2 g. The combination of the NMDA receptor blocker APV (50 microM) and the AMPA/kainate (KA) receptor blocker CNQX (10 microM) resulted in significantly improved recovery of CAP amplitude postinjury; however, the NMDA receptor antagonist APV alone did not enhance postinjury recovery, and infusion of NMDA (10 microM) did not affect recovery of the CAPs. In contrast, the AMPA/KA receptor blockers NBQX (10 microM) or CNQX (10 microM) significantly enhanced the recovery of CAP amplitude postinjury. The agonists AMPA (100 microM) or KA (100 microM) resulted in significant attenuation of CAP amplitude postinjury. Coapplication of AMPA/KA plus NBQX and CNQX was also associated with improved functional recovery. After incubation with AMPA and KA, Co(2+)-positive glia were visualized in spinal cord white matter. Similar results were seen after compressive injury but not in control cords. Immunohistochemistry and Western blot analysis demonstrated AMPA (GluR4)- and KA (GluR6/7 and KA2)-positive astrocytes in spinal cord white matter. In summary, non-NMDA ionotropic glutamate receptors seem to be involved in the pathophysiology of traumatic spinal cord injury. The presence of AMPA (GluR4) and KA (GluR6/7 and KA2) receptors on periaxonal astrocytes suggests a role for these cells in glutamatergic white matter injury.
Figures
References
-
- Agrawal SK, Fehlings MG. Mechanisms of calcium mediated axonal injury after spinal cord trauma. Soc Neurosci Abstr. 1995;21:381.
-
- Barres BA, Koroshetz WJ, Swartz KJ, Chun LLY, Corey DP. Ion channel expression by white matter glia: the O-2A glial progenator cell. Neuron. 1990;4:507–524. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous