

Association between blood lactate and acid-base status and mortality in ventilated babies
- PMID: 9059180
- PMCID: PMC1720617
- DOI: 10.1136/fn.76.1.f15
Association between blood lactate and acid-base status and mortality in ventilated babies
Abstract
Aim: To investigate the relation between common acid-base parameters and blood lactate concentrations and their prognostic importance in sick, ventilated neonates.
Methods: Two hundred and seventy eight serial simultaneous measurements of arterial acid-base status and blood lactate concentrations were carried out in 75 mechanically ventilated neonates with indwelling arterial catheters (gestational age and birthweight, median (range) -29 (23-40) weeks, and 1340 (550-4080) g, respectively).
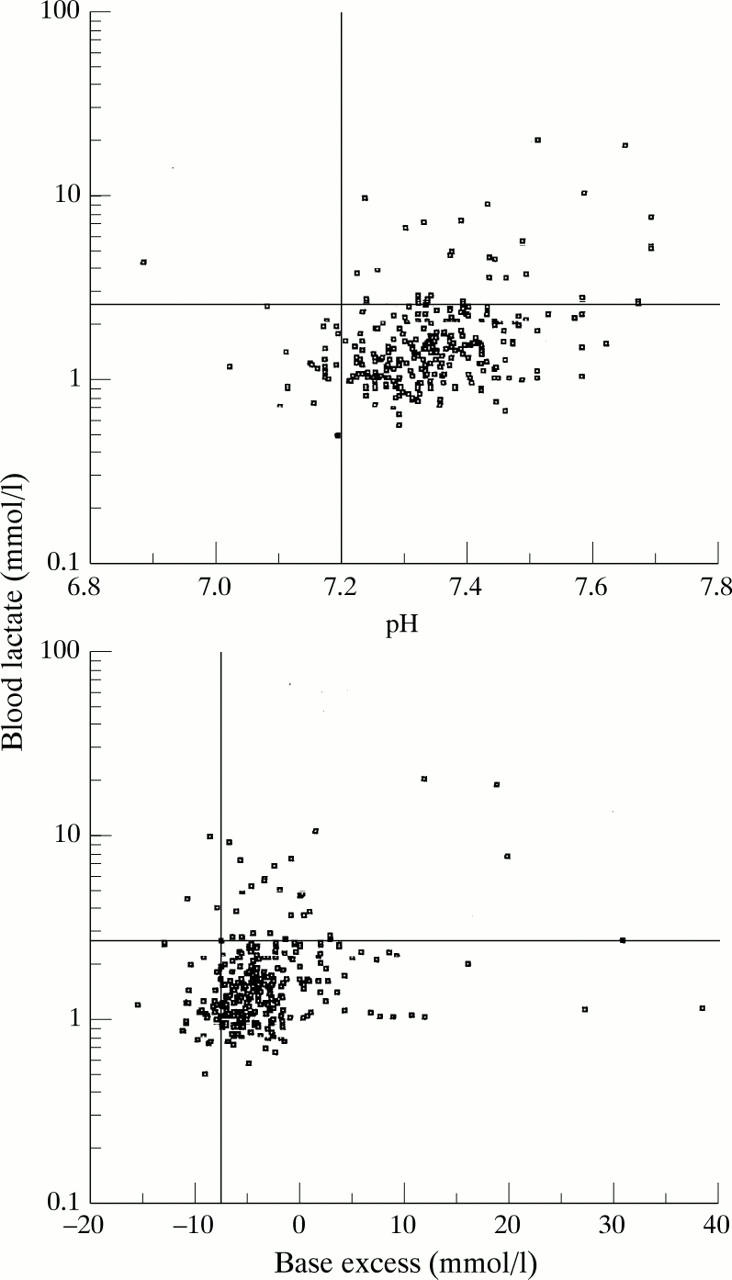
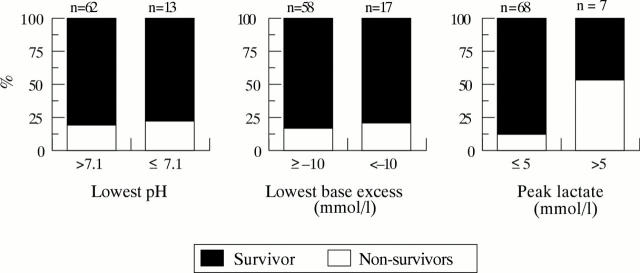
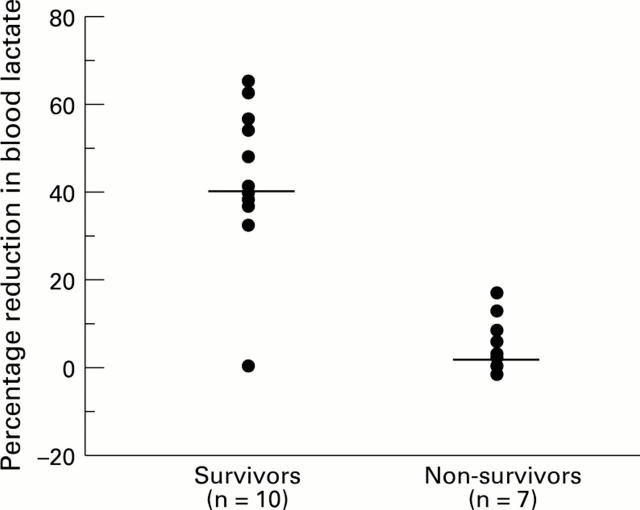
Results: There were no correlations between arterial blood lactate and pH and base excess within subjects (r = 0.07 and r = -0.06, respectively) and only weakly positive but clinically irrelevant positive correlations between subjects (r = 0.28 and r = 0.27) in this group. Even in those infants who had not received any bicarbonate before their initial measurements (n = 48), there were no correlations between initial blood lactate concentrations and pH (r = 0.27), base excess (r = 0.17), or serum bicarbonate concentrations (r = -0.18). There was no relation between peak lactate concentration (PLC) and base excess (r = 0.16), and only a weak correlation between peak lactate concentration (PLC) and pH (r = 0.28). Negative base excess was an insensitive indicator of raised lactate concentrations. Only two out of 33 (6%) instances of hyperlactataemia (lactate > 2.5 mmol/l) would have been identified with a base excess < -10 mmol/l as a cutoff. Lower cutoff values of base excess or pH performed no better. Raised lactate concentrations were associated with increased mortality at all levels. While six of 53 (11%) infants with a PLC < 2.5 mmol/l died, this proportion increased to four of 15 (27%) with a PLC between 2.5-5.0 mmol/l, and four of seven (57%) with a PLC > 5.0 mmol/l. Infants showing little rise or a substantial fall in blood lactate fared better than those with persistently raised values. A clinically important increase in blood lactate preceded the development of clinical markers of deterioration and complications in six infants.
Conclusions: Contrary to popular belief, pH or base excess cannot be used as proxy measures for blood lactate concentration, and independent measurement of the latter are needed. Blood lactate concentrations may provide an early warning signal and important prognostic information in ill, ventilated neonates. In this regard, serial measurements of blood lactate are more useful than a single value.
Figures
Comment in
-
Lactate and anion gap in asphyxiated neonates.Arch Dis Child Fetal Neonatal Ed. 1998 Jan;78(1):F80. doi: 10.1136/fn.78.1.f78d. Arch Dis Child Fetal Neonatal Ed. 1998. PMID: 9536852 Free PMC article. No abstract available.