

Variations of posterior vitreous detachment
- PMID: 9290361
- PMCID: PMC1722241
- DOI: 10.1136/bjo.81.7.527
Variations of posterior vitreous detachment
Abstract
Aims: To identify variations in posterior vitreous detachment (PVD) and establish a clinical classification system for PVD.
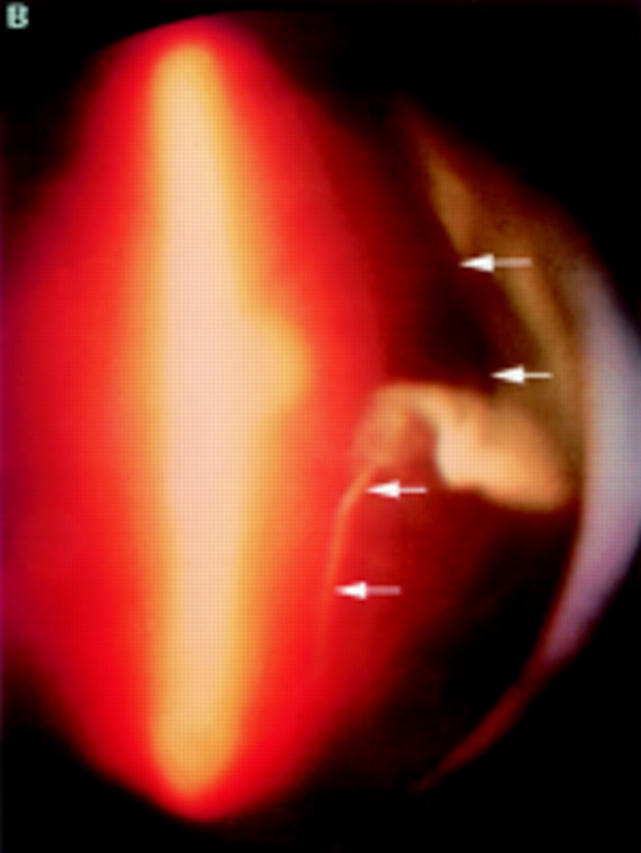
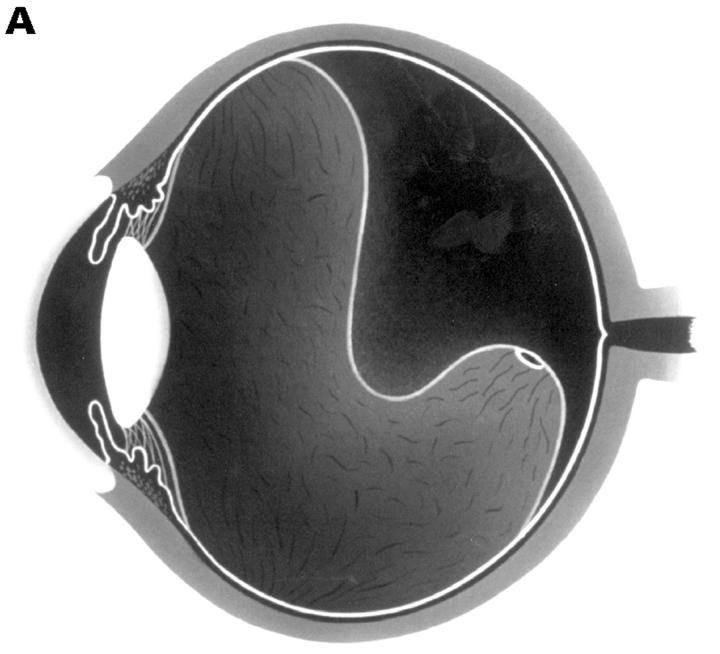
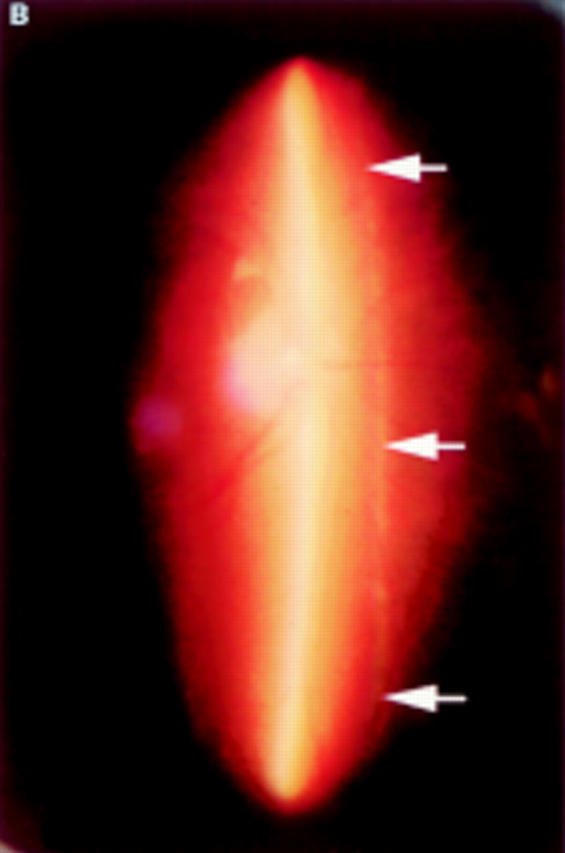
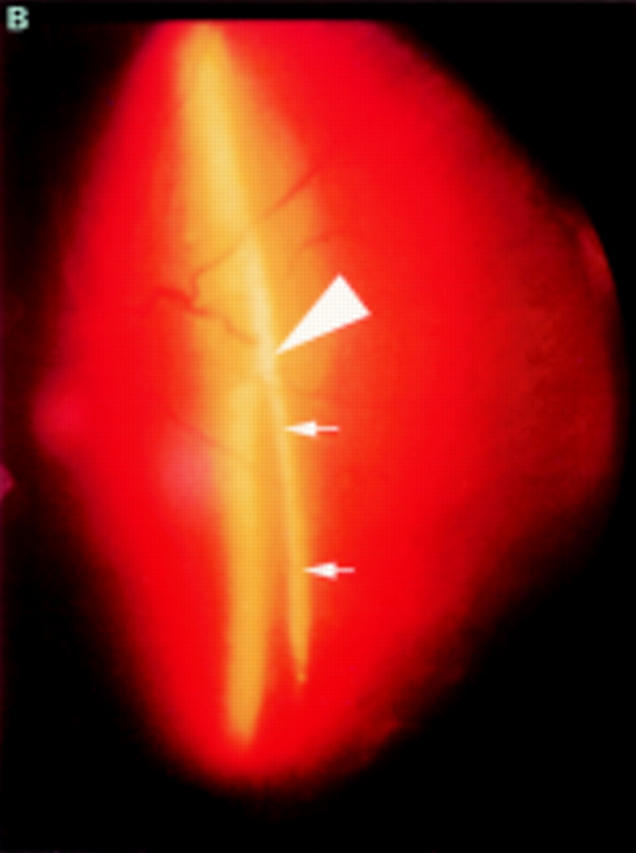
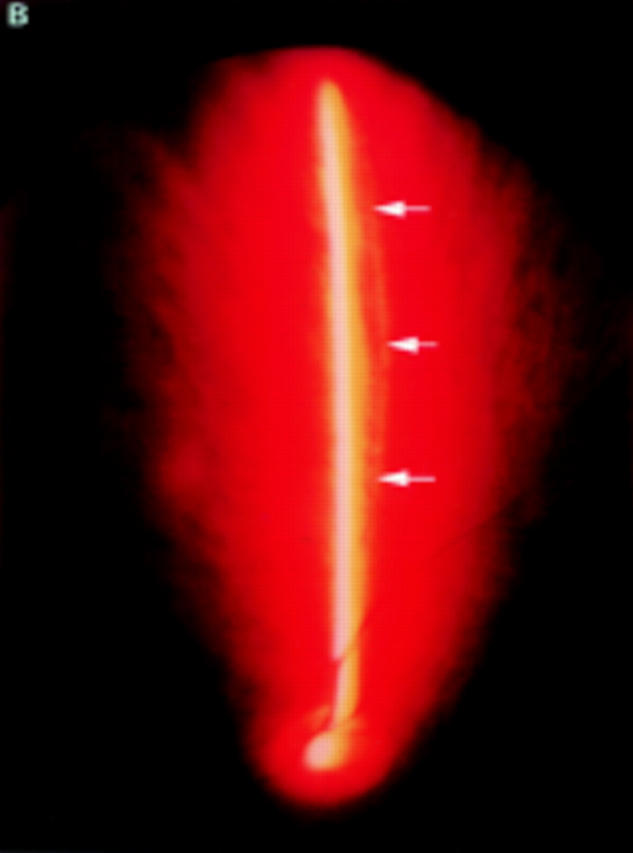
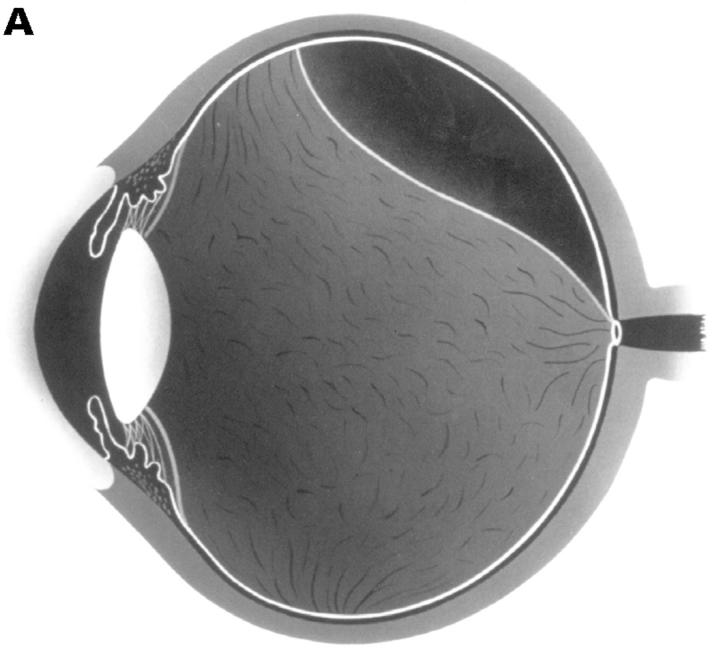
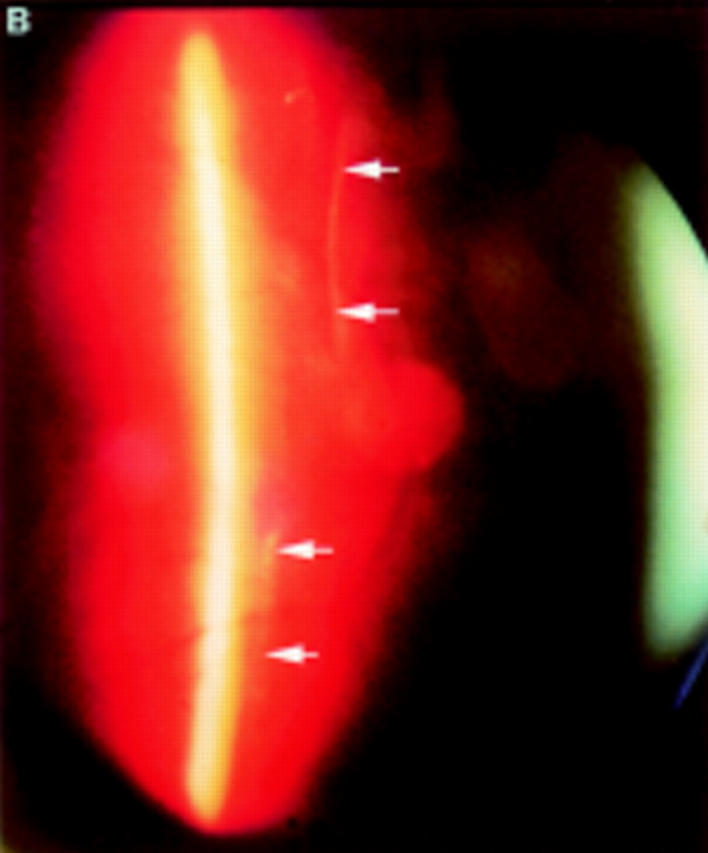
Methods: 400 consecutive eyes were examined using biomicroscopy and vitreous photography and classified the PVD variations-complete PVD with collapse, complete PVD without collapse, partial PVD with thickened posterior vitreous cortex (TPVC), or partial PVD without TPVC.
Results: In each PVD type, the most frequently seen ocular pathologies were as follows: in complete PVD with collapse (186 eyes), age related changes without vitreoretinal diseases (77 eyes, 41.4%) and high myopia (55 eyes, 29.6%); in complete PVD without collapse (39 eyes), uveitis (23 eyes, 59.0%) and central retinal vein occlusions (8 eyes, 20.5%); in partial PVD with TPVC (64 eyes), proliferative diabetic retinopathy (30 eyes, 46.9%); and inpartial PVD without TPVC (111 eyes), age related changes without vitreoretinal diseases (62 eyes, 55.9%). This PVD categorisation was significantly associated with the prevalence of each vitreoretinal disease (p < 0.0001, chi 2 test on contingency table).
Conclusions: PVD variations can be classified into four types, which is clinically useful because each type corresponds well to specific vitreoretinal changes.
Figures



Comment in
-
Classifying posterior vitreous detachment: a new way to look at the invisible.Br J Ophthalmol. 1997 Jul;81(7):521. doi: 10.1136/bjo.81.7.521. Br J Ophthalmol. 1997. PMID: 9290358 Free PMC article. No abstract available.
References
-
- Arch Ophthalmol. 1965 Dec;74(6):741-51 - PubMed
-
- Graefes Arch Clin Exp Ophthalmol. 1995 Jul;233(7):430-4 - PubMed
-
- Arch Ophthalmol. 1966 Feb;75(2):238-46 - PubMed
-
- Trans Am Acad Ophthalmol Otolaryngol. 1967 Jul-Aug;71(4):642-52 - PubMed
-
- Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1975;193(1):33-56 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources