

Pregnancy after liver transplantation under tacrolimus
- PMID: 9293865
- PMCID: PMC2975612
- DOI: 10.1097/00007890-199708270-00002
Pregnancy after liver transplantation under tacrolimus
Abstract
Background: The maternal and fetal risk of pregnancy after organ transplantation under tacrolimus has not been reported. This was prospectively studied in 27 pregnancies by 21 female liver recipients who were treated with tacrolimus before and throughout gestation.
Method: Twenty-seven babies were born between October 1990 and April 1996. In 15 cases, samples were obtained at or after delivery and stored (-40 degrees C) for comparison of tacrolimus concentration in the maternal blood with different combinations of cord and infant venous blood, breast milk, or a section of the placenta.
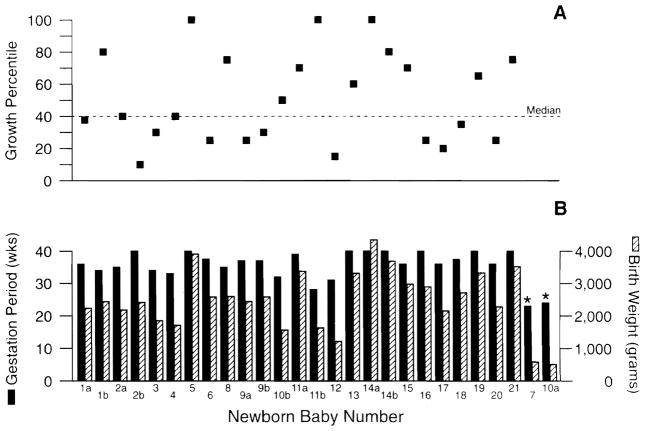
Results: The 21 mothers had surprisingly few serious complications of pregnancy and no mortality. Two infants with 23 and 24 weeks gestation died shortly after birth. The mean birth weight of the other 25 was 2638+/-781 g after a gestational period of 36.6+/-3.3 weeks. Mean birth weight percentile for gestational age was 50.2+/-26.2 (median 40). On the day of delivery, the mean tacrolimus concentrations (ng/ml) were 4.3 in placenta versus 1.5, 0.7, and 0.5 in maternal, cord, and child plasma, and 0.6 in the first breast milk specimens. The infants had a 36% incidence of transient perinatal hyperkalemia (K+>7.0 meq/L) and a mild reversible renal impairment, which were thought to reflect in part maternal homeostasis. One newborn had unilateral polycystic renal disease (the only anomaly). All 25 babies have had satisfactory postnatal growth and development with a current mean weight percentile of 62+/-37 (median 80).
Conclusions: Pregnancy by postliver transplant mothers under tacrolimus was possible with a surprisingly low incidence of the hypertension, preeclampsia, and other maternal complications historically associated with such gestations. As in previous experience with other immunosuppressive regimens, preterm deliveries were common. However, prenatal growth for gestational age and postnatal infant growth for postpartum age were normal.
Figures
Comment in
-
Tacrolimus and breastfeeding.Transplantation. 1998 Mar 27;65(6):864. doi: 10.1097/00007890-199803270-00016. Transplantation. 1998. PMID: 9539100 No abstract available.
-
Comment on "Pregnancy after liver transplantation under tacrolimus" by Jain et al.Transplantation. 1998 May 27;65(10):1415-6. doi: 10.1097/00007890-199805270-00027. Transplantation. 1998. PMID: 9625033 No abstract available.
References
-
- Penn I, Makowski EL, Harris P. Parenthood following renal and hepatic transplantation. Transplantation. 1980;30:397. - PubMed
-
- Laifer SA, Darby MJ, Scantlebury VP, Harger JH, Caritis SN. Pregnancy and liver transplantation. Obstet Gynecol. 1990;76(6):1083. - PubMed
-
- Radomski JS, Ahlswede BA, Jarrell BE, et al. Outcomes of 500 pregnancies in 335 female kidney, liver, and heart transplant recipients. Transplant Proc. 1995;27(1):1089. - PubMed
-
- Radomski JS, Moritz MJ, Munoz SJ, Cater JR, Jarrell BE, Armenti VT. National Transplantation Pregnancy Registry: analysis of pregnancy outcomes in female liver transplant recipients. Liver Transplant Surg. 1995;1(5):281. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
