

Early gastric cancer in Europe
- PMID: 9301490
- PMCID: PMC1891459
- DOI: 10.1136/gut.41.2.142
Early gastric cancer in Europe
Abstract
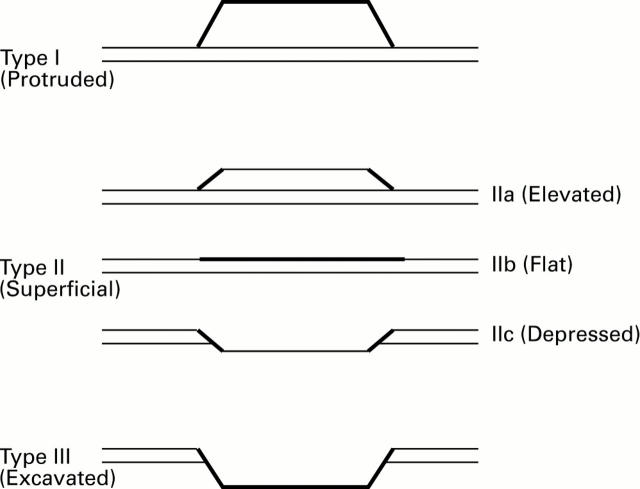
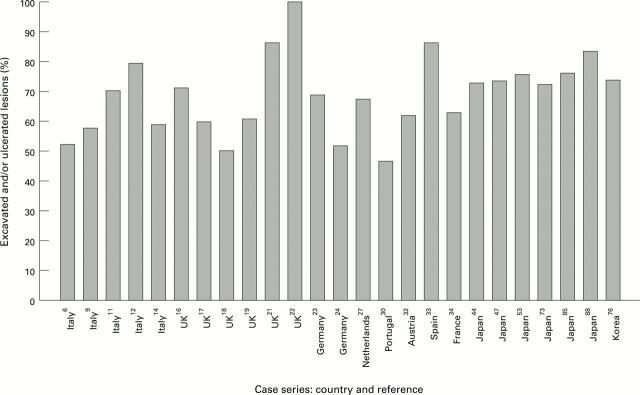
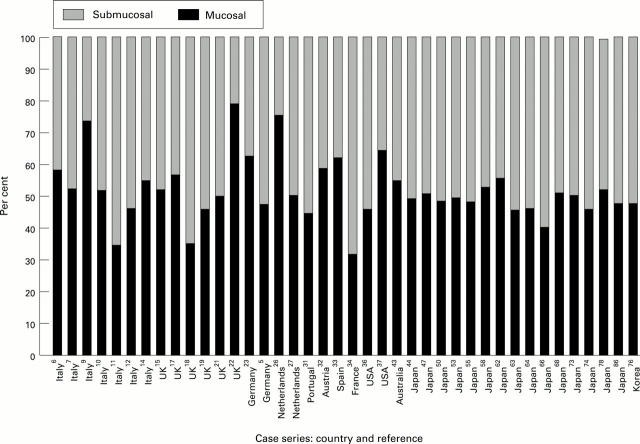
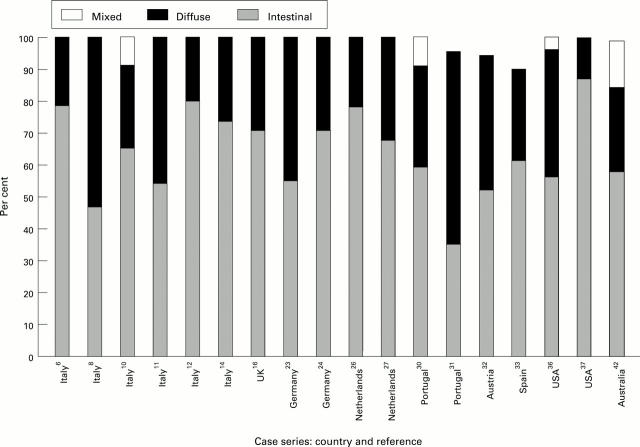
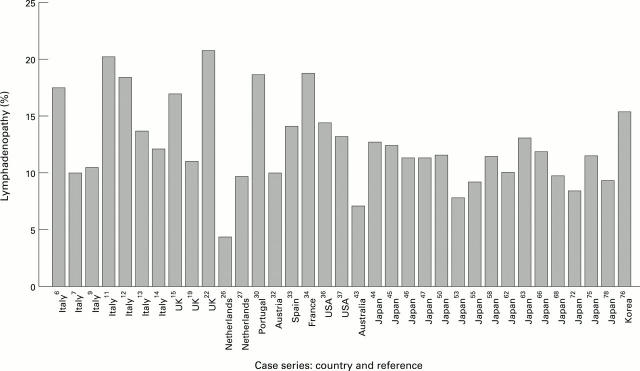
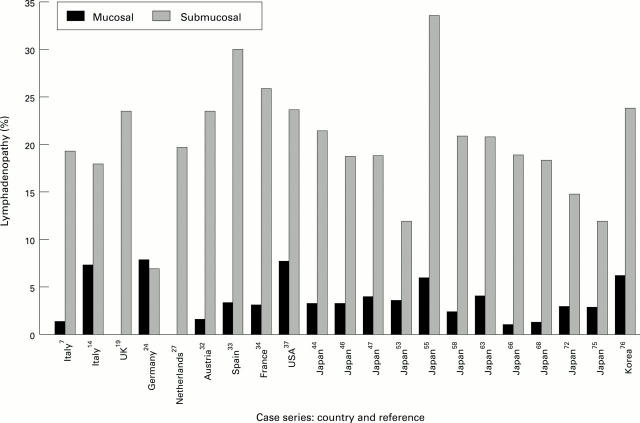
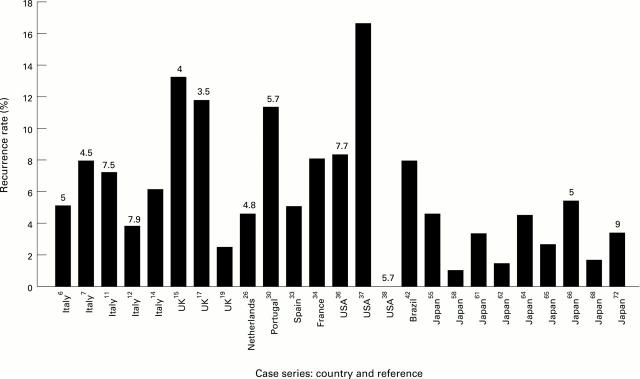
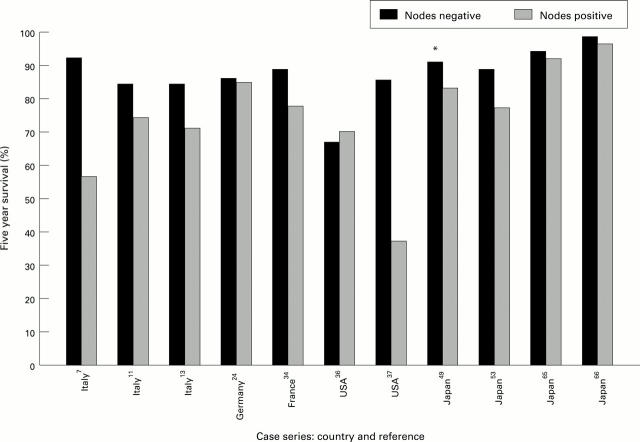
Despite mass population screening and an incidence of EGC in Japan that is at least double that of the West, there seem to be no genuine differences in the clinicopathological features of the disease between the two regions. The macroscopic appearance, size, depth of invasion, frequency of lymph node invasion, and histology of EGC are all remarkably similar in Japan, Europe and America, as are sex and age distributions. Patients with EGC are a number of years younger than those with advanced cancer. This is not surprising: Tsukuma et al followed 56 cases of EGC that were not surgically treated and estimated that the median "duration of EGC" before becoming advanced was 37 months. This suggests that EGC undergoes a period of slow growth before becoming advanced. Further differences between early and advanced cancers include a higher frequency of synchronous cancers and a longer symptom duration in EGC. Unfavourable prognostic factors in EGC include lymph node invasion, and invasion through the muscularis mucosae, though it is not clear whether these are independent. Repeated attempts have been made to identify other prognostic factors, but no clear pattern has emerged, with the possible exceptions of patient age, tumour size, and the presence of ulceration. The postsurgical outcome of EGC in the West is marginally less favourable than in Japan. In view of the similar clinical and pathological features in the two regions it seems likely, therefore, that this is because of the more aggressive surgical techniques traditionally used in Japan. Conversely, however, EMR has recently emerged as an important technique in Japan. Despite the advantages of low operative mortality and normal function of the postoperative stomach, there are also a number of potential disadvantages. It would seem sensible, therefore, to await the results of long term follow up studies before widespread adoption of EMR in Europe. Nevertheless, this technique should be considered for frail patients unfit for more radical surgery.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical