

Diffuse oesophageal spasm: diagnosis by ambulatory 24 hour manometry
- PMID: 9301491
- PMCID: PMC1891460
- DOI: 10.1136/gut.41.2.151
Diffuse oesophageal spasm: diagnosis by ambulatory 24 hour manometry
Abstract
Background: Diffuse oesophageal spasm (DOS) is a potential cause of intermittent chest pain and/or dysphagia. In the past, the diagnosis of DOS has relied on criteria obtained from standard oesophageal manometry (more than one simultaneous contraction in a series of 10 wet swallows with the rest being peristaltic). As symptoms are intermittent, however, 24 hour manometry may well be more suited to its investigation.
Aims: To determine the ability of 24 hour manometry to detect the symptomatic contractions of DOS and to compare standard, laboratory based manometry with 24 hour manometry in its diagnosis.
Patients: Three hundred and ninety consecutive patients referred with suspected oesophageal disorders.
Methods: Standard laboratory based manometry and 24 hour outpatient manometry.
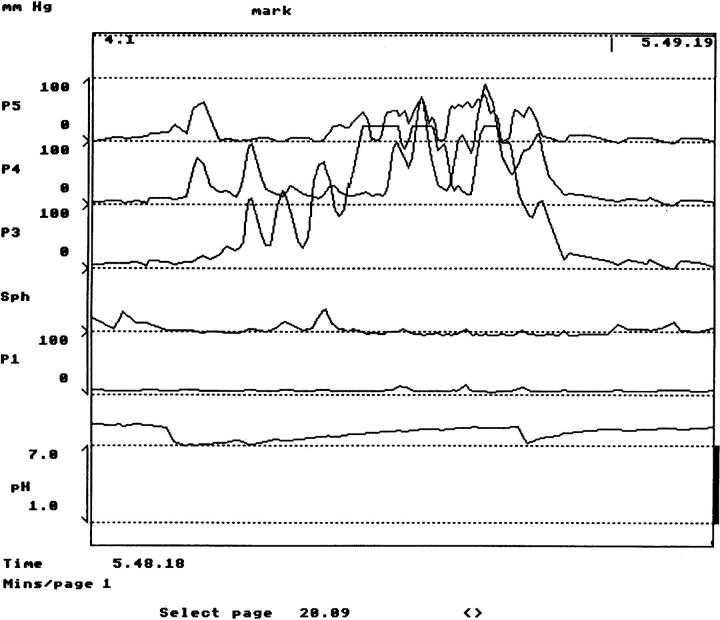
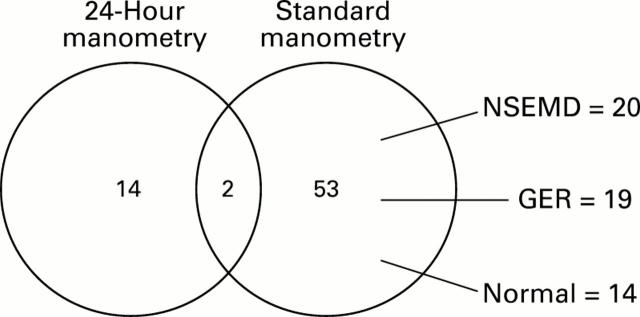
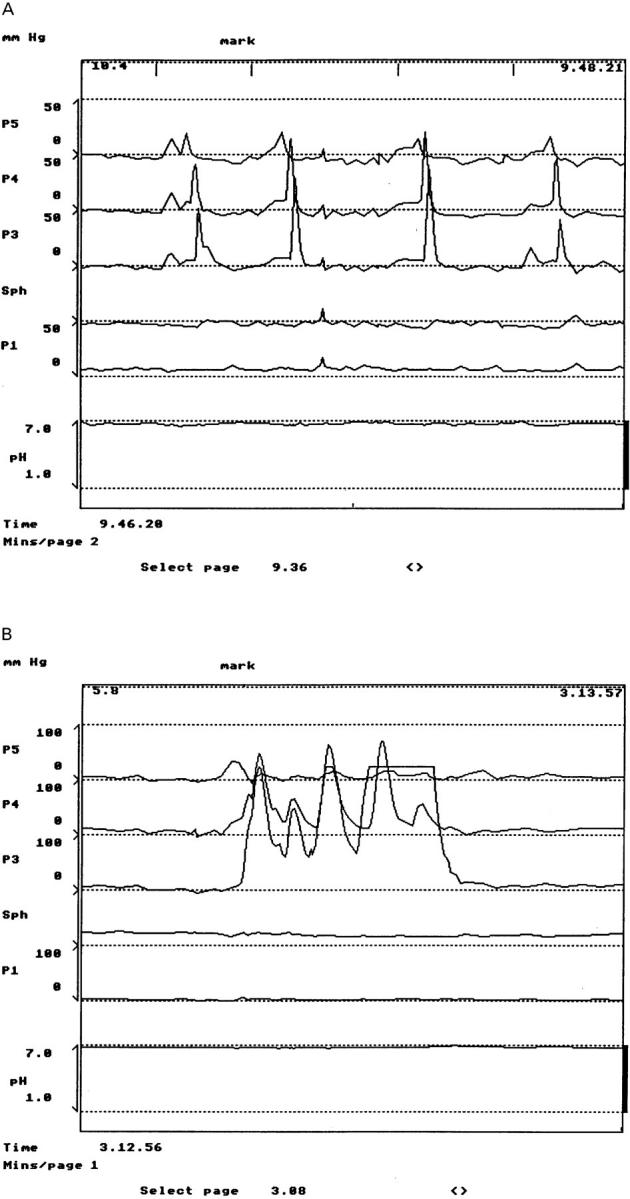
Results: Sixteen patients were classified by 24 hour manometry as having DOS on the basis of painful contractions (spasms) of excessive duration and increased amplitude. Laboratory based manometry failed to detect the majority of these patients with DOS (14/16), and 53/55 were incorrectly labelled as having DOS on the basis of asymptomatic manometric findings.
Conclusion: The detection of symptomatic DOS requires 24 hour manometry.
Figures
Similar articles
-
Clinical and manometric aspects of diffuse esophageal spasm in a cohort of subjects evaluated for dysphagia and/or chest pain.Am J Med Sci. 1990 Sep;300(3):148-51. doi: 10.1097/00000441-199009000-00004. Am J Med Sci. 1990. PMID: 2240005
-
Diagnostic yield of 24-hour esophageal manometry in non-cardiac chest pain.Neurogastroenterol Motil. 2016 Aug;28(8):1186-93. doi: 10.1111/nmo.12818. Epub 2016 Mar 27. Neurogastroenterol Motil. 2016. PMID: 27018150
-
Ambulatory oesophageal manometry and pH monitoring for investigation of chest pain: a New Zealand experience.N Z Med J. 2006 Mar 10;119(1230):U1877. N Z Med J. 2006. PMID: 16532043
-
Spasm, nutcracker, and IEM: real or manometry findings?J Clin Gastroenterol. 2008 May-Jun;42(5):647-51. doi: 10.1097/MCG.0b013e3181646d19. J Clin Gastroenterol. 2008. PMID: 18364582 Review.
-
Current concepts on pathophysiology, diagnosis and treatment of diffuse oesophageal spasm.Drugs. 2001;61(5):579-91. doi: 10.2165/00003495-200161050-00004. Drugs. 2001. PMID: 11368284 Review.
Cited by
-
Oesophageal surgery.World J Gastroenterol. 2001 Dec;7(6):760-5. doi: 10.3748/wjg.v7.i6.760. World J Gastroenterol. 2001. PMID: 11854896 Free PMC article. Review. No abstract available.
-
A review of oesophageal manometry testing in a district general hospital.Postgrad Med J. 2002 Jan;78(915):34-6. doi: 10.1136/pmj.78.915.34. Postgrad Med J. 2002. PMID: 11796870 Free PMC article.
-
Functional aspects of distal oesophageal spasm: the role of onset velocity and contraction amplitude on bolus transit.Dig Liver Dis. 2012 Jul;44(7):569-75. doi: 10.1016/j.dld.2012.02.003. Epub 2012 Apr 3. Dig Liver Dis. 2012. PMID: 22475443 Free PMC article.
-
High-Resolution Manometry in Clinical Practice.Gastroenterol Hepatol (N Y). 2015 Jun;11(6):374-84. Gastroenterol Hepatol (N Y). 2015. PMID: 27118931 Free PMC article.
-
Comparison of the esophageal manometric characteristics of idiopathic and reflux-associated esophageal spasm: evaluation by 24-hour ambulatory esophageal motility and pH monitoring.Dig Dis Sci. 2003 Nov;48(11):2124-31. doi: 10.1023/b:ddas.0000004514.91064.7f. Dig Dis Sci. 2003. PMID: 14705816
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous