

Reduced incidence and delayed onset of diabetes in perforin-deficient nonobese diabetic mice
- PMID: 9314549
- PMCID: PMC2199062
- DOI: 10.1084/jem.186.7.989
Reduced incidence and delayed onset of diabetes in perforin-deficient nonobese diabetic mice
Abstract
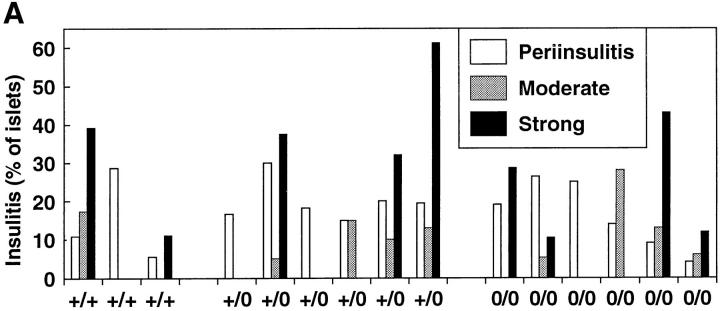
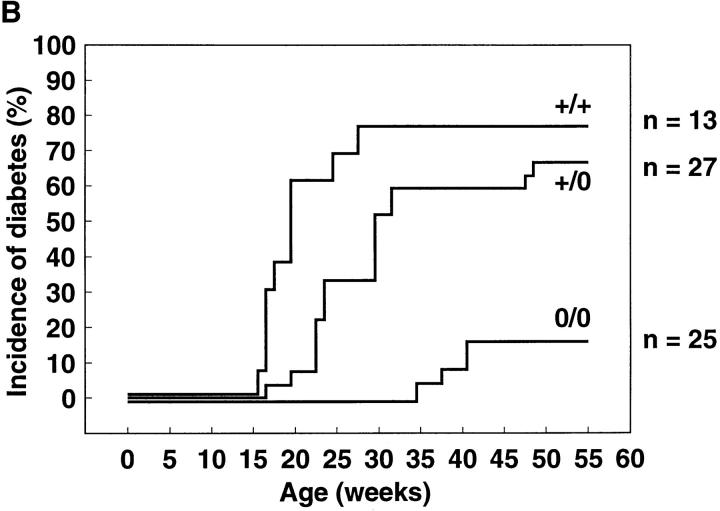
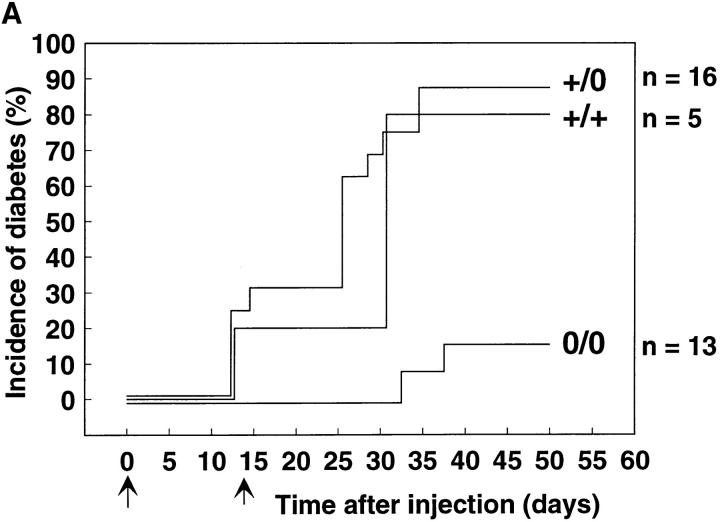
To investigate the role of T cell-mediated, perforin-dependent cytotoxicity in autoimmune diabetes, perforin-deficient mice were backcrossed with the nonobese diabetes mouse strain. It was found that the incidence of spontaneous diabetes over a 1 yr period was reduced from 77% in perforin +/+ control to 16% in perforin-deficient mice. Also, the disease onset was markedly delayed (median onset of 39.5 versus 19 wk) in the latter. Insulitis with infiltration of CD4(+) and CD8(+) T cells occurred similarly in both groups of animals. Lower incidence and delayed disease onset were also evident in perforin-deficient mice when diabetes was induced by cyclophosphamide injection. Thus, perforin-dependent cytotoxicity is a crucial effector mechanism for beta cell elimination by cytotoxic T cells in autoimmune diabetes. However, in the absence of perforin chronic inflammation of the islets can lead to diabetogenic beta cell loss by less efficient secondary effector mechanisms.
Figures





References
-
- Makino S, Kunimoto K, Muraoka Y, Mizushima Y, Katagiri K, Tochino Y. Breeding of a non-obese diabetic strain of mice. Exp Anim (Tokyo) 1980;29:1–13. - PubMed
-
- Miller BJ, Appel MC, O'Neil JJ, Wicker LS. Both the Lyt-2+ and L3T4+T cell subsets are required for the transfer of diabetes in nonobese diabetic mice. J Immunol. 1988;140:52–58. - PubMed
-
- Bradley BJ, Haskins K, La FG, Rosa, Lafferty KJ. CD8 T cells are not required for islet destruction induced by a CD4-positive islet-specific T cell clone. Diabetes. 1992;41:1603–1608. - PubMed
-
- Katz JD, Benoist C. T helper cell subsets in insulin-dependent diabetes. Science (Wash DC) 1995;268:1185–1188. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
