

Evaluating treatment protocols to prevent antibiotic resistance
- PMID: 9342370
- PMCID: PMC23718
- DOI: 10.1073/pnas.94.22.12106
Evaluating treatment protocols to prevent antibiotic resistance
Abstract
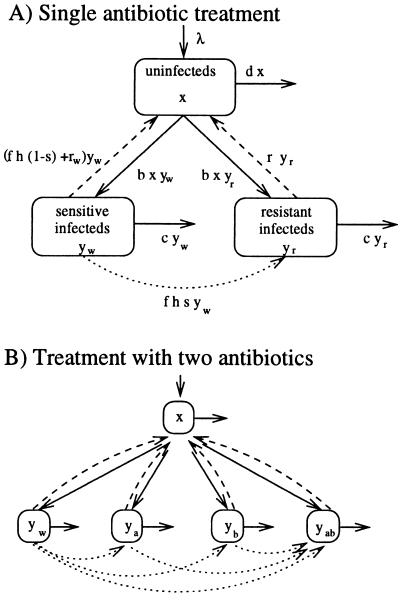
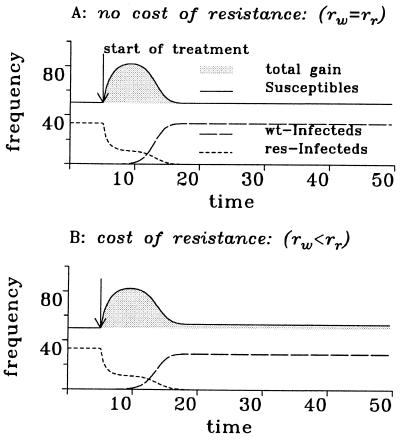
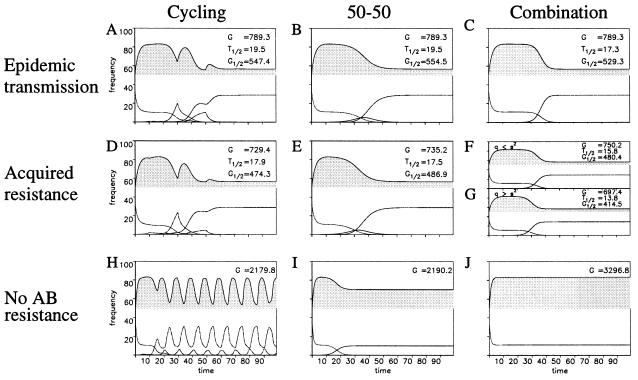
The spread of bacteria resistant to antimicrobial agents calls for population-wide treatment strategies to delay or reverse the trend toward antibiotic resistance. Here we propose new criteria for the evaluation of the population-wide effects of treatment protocols for directly transmitted bacterial infections and discuss different usage patterns for single and multiple antibiotic therapy. A mathematical model suggests that the long-term benefit of single drug treatment from introduction of the antibiotic until a high frequency of resistance precludes its use is almost independent of the pattern of antibiotic use. When more than one antibiotic is employed, sequential use of different antibiotics in the population ("cycling") is always inferior to treatment strategies where, at any given time, equal fractions of the population receive different antibiotics. However, treatment of all patients with a combination of antibiotics is in most cases the optimal treatment strategy.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
