

Automated evidence-based critiquing of orders for abdominal radiographs: impact on utilization and appropriateness
- PMID: 9391938
- PMCID: PMC61269
- DOI: 10.1136/jamia.1997.0040511
Automated evidence-based critiquing of orders for abdominal radiographs: impact on utilization and appropriateness
Abstract
Objective: Inappropriate utilization of diagnostic testing has been well documented. The purpose of this study was to measure the impact of presenting real time, evidence-based critiques about the appropriateness of abdominal radiograph (KUB) orders on physician decision making.
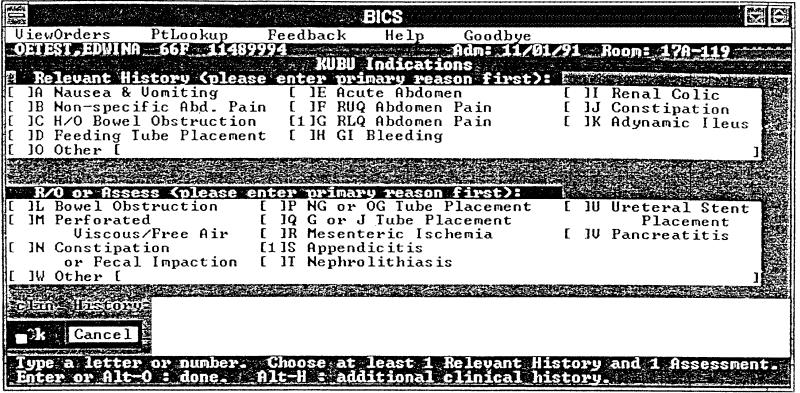
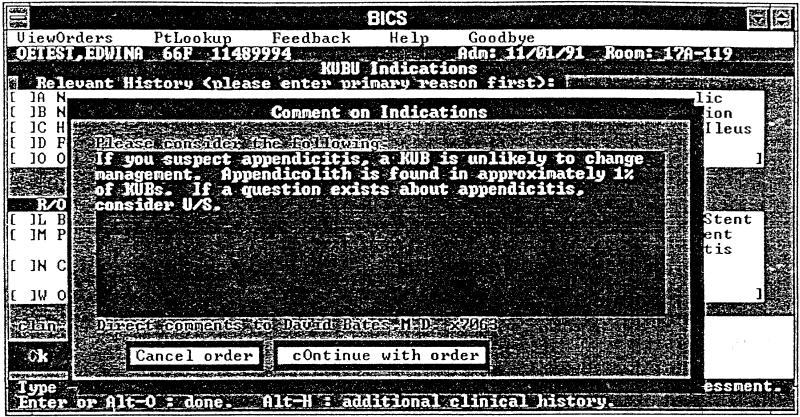
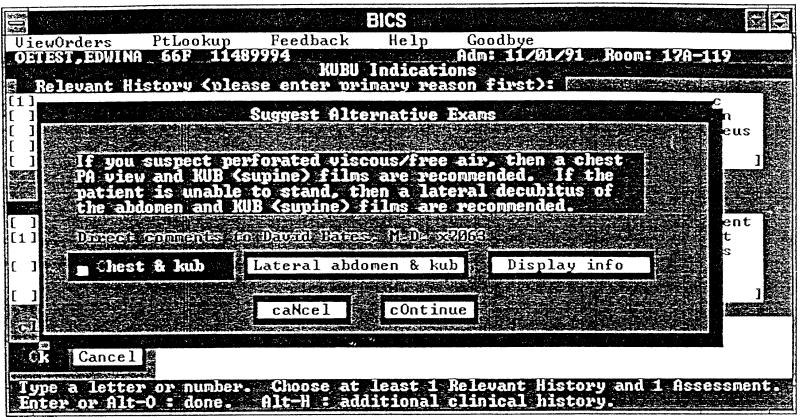
Design: Prospective trial where evidence-based critiques were presented to ordering clinicians in two kinds of situations: (1) a KUB was likely to have a low probability of providing useful information, or (2) an alternative view(s) was more appropriate given the clinical circumstance. There were two phases of the trial: Phase 1 was a 9-week period where evidence-based critiques were presented at the time of ordering a KUB, followed by Phase 2, a 19-week period in which orderers were randomized to receive critiques either amended to include both institutional data regarding the utility of the critiques and stronger messages about the lack of utility of the study, or the same critiques as presented in Phase 1, depending upon indication. Based upon the radiologist's report of their interpretation of the exams, the results of the examinations were scored as positive, equivocal, or negative using structured criteria.
Results: 299 KUBs in Phase 1 and 385 KUBs in Phase 2 received at least one critique. Cancellation rates of low yield films were low, and were similar in Phase 1 and 2, 8/258 (3%) vs. 10/283 (4%). Compliance with the recommendation for alternative view(s) was higher: 19/104 (38%) in Phase 1 vs. 96/176 (55%) in Phase 2 (p = 0.006). The results differentiated low-yield from non-low-yield films: 5% of low-yield films vs. 20% of non-low-yield films were positive in Phase 2 (p < 0.0001). Surgical physicians were less likely to cancel (p = 0.07) or to change to the suggested view(s) (p < 0.0001) than medical physicians or nurses.
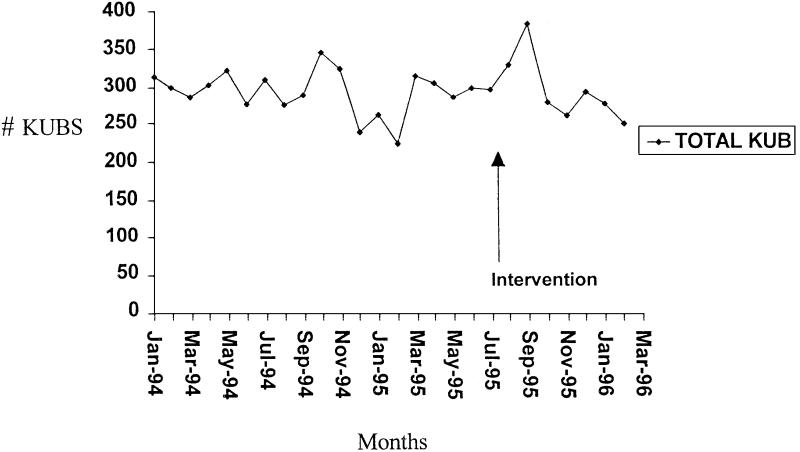
Conclusions: The intervention identified clinical situations in which KUBs appeared to have a low clinical yield. In response to evidence-based critiques, providers were reluctant to cancel their order, but were more willing to change to different views. To reduce the number of inappropriate radiographic films, stronger incentives or interventions may be required.
Figures
References
-
- Schroeder SA, Kenders K, Cooper JK, Piemme TE. Use of laboratory tests and pharmaceuticals: variation among physicians and effect of cost audit on subsequent use. JAMA. 1973;225: 969-73. - PubMed
-
- Eisenberg JM, Williams SV, Garner L, Viale R, Smits H. Computer-based audit to detect and correct overutilization of laboratory tests. Med Care. 1977;15: 915-21. - PubMed
-
- Williams SV, Eisenberg JM. A controlled trial to decrease the unnecessary use of diagnostic tests. J Gen Intern Med. 1986;1: 8-13. - PubMed
-
- Dixon RH, Laszle J. Utilization of clinical chemistry services by medical house staff. An analysis. Arch Intern Med. 1974;134: 1064-7. - PubMed
-
- Tierney WM, McDonald CJ, Hui SL, Martin DK. Computer predictions of abnormal results: effects on outpatient testing. JAMA. 1988;259: 1194-8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
