

Macroaspartasemia as a cause of isolated elevation of aspartate aminotransferase--its biochemical and physiological characteristics
- PMID: 9439157
- PMCID: PMC4531981
- DOI: 10.3904/kjim.1997.12.2.208
Macroaspartasemia as a cause of isolated elevation of aspartate aminotransferase--its biochemical and physiological characteristics
Abstract
Objectives: The increase of serum aspartate aminotransferase (AST) is generally found in hepatic, cardiac, muscular disease and hemolytic disorders of the red blood cell (RBC). The elevation of its activity is suspected in pathological conditions of these organs. However, instances without any of those conditions rarely exist.
Methods: The experimental samples were obtained from a normal person's hemolysed RBC, a hepatitis patient and a macroaspartatemic female's serum. They were studied with exclusion chromatography, electrophoresis of AST and changes of AST activity due to Polyethylene Glycol (PEG) and various conditions on storage.
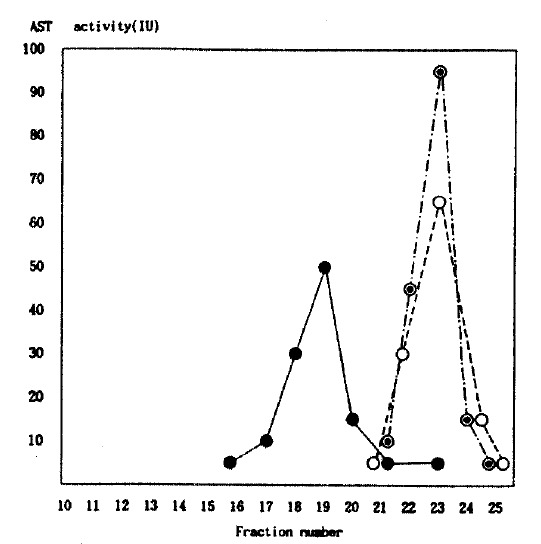
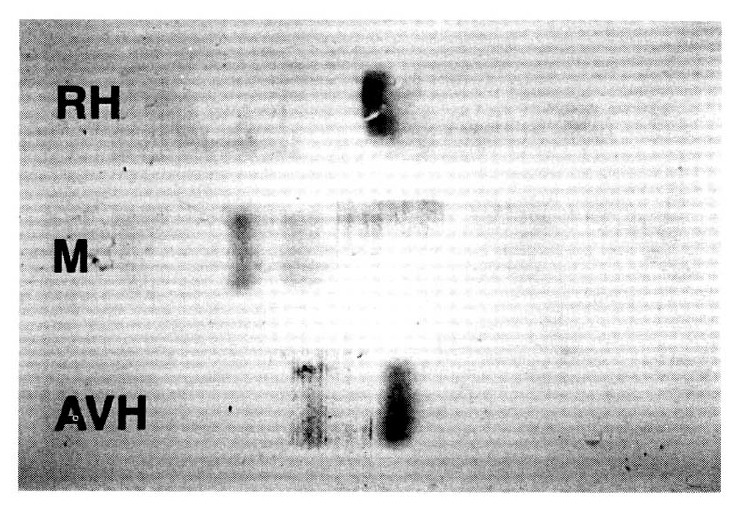
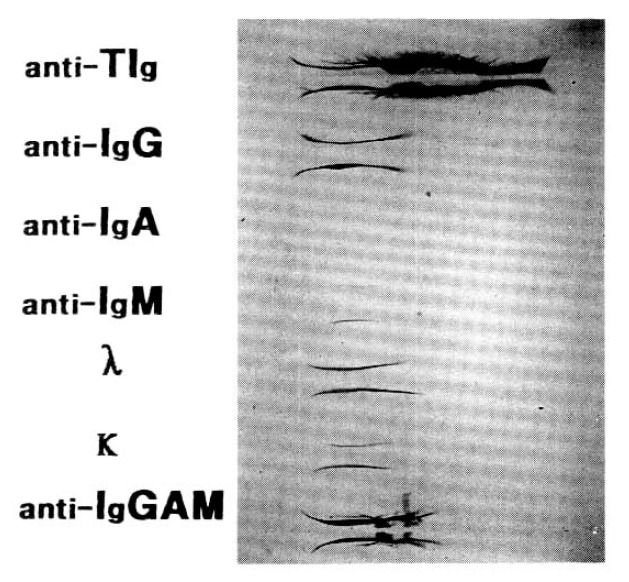
Results: 1) The patterns of AST activity by exclusion chromatography are similar to the hemolysed RBC and the hepatitis's serum but differs by the isolated AST elevation. 2) The AST activity with addition of PEG and different anti-immunoglobulin subtypes to different serums are slightly decreased in hepatitis but markedly decreased with PEG and anti-IgG in macroaspartatemia. 3) The patterns of AST activity in electrophoresis are single band-cytosomal AST (cAST)-from hemolysed RBC and two bands-mitochondrial AST (mAST) and cAST-from hepatitis, the major being cAST and the minor mAST. Even though there are two bands, the major one is atypical and the minor corresponds to mAST in macroaspartatemia. 4) The changes of AST activity on storage according to time and temperature show to be stable over 4 weeks at room temperature and cooled condition, and 9 weeks under frozen state in macroaspartatase.
Conclusion: Concluding from the above findings, macroaspartatemia is an enzyme-immunoglobulin complex composed of cAST with IgG. MacroAST might be stabler than usual AST at physical conditions.
Figures
Similar articles
-
Aspartate aminotransferase macroenzyme complex in serum identified and characterized.Clin Chem. 1994 Jul;40(7 Pt 1):1340-3. Clin Chem. 1994. PMID: 8013110
-
Immunoglobulin-complexed aspartate aminotransferase.Intern Med. 1993 Feb;32(2):156-9. doi: 10.2169/internalmedicine.32.156. Intern Med. 1993. PMID: 8507927
-
Investigation of a persistently raised serum AST.Ann Clin Biochem. 1989 Nov;26 ( Pt 6):538-41. doi: 10.1177/000456328902600614. Ann Clin Biochem. 1989. PMID: 2619234
-
Persistent Isolated Elevation of Aspartate Aminotransferase in an Asymptomatic Female Patient: a Case Report and Review of Current Literature.Clin Lab. 2019 Aug 1;65(8). doi: 10.7754/Clin.Lab.2019.190205. Clin Lab. 2019. PMID: 31414761 Review.
-
[Macroaspartate aminotransferase. Study of 5 cases and review of the literature].Gastroenterol Clin Biol. 1998 May;22(5):549-53. Gastroenterol Clin Biol. 1998. PMID: 9762295 Review. French.
References
-
- Stolz A, Kaplowitz N. Biochemical tests for liver disease. In: Zakim D, Boyer TD, editors. Hepatology; A textbook of liver disease. 2nd ed. Philadelphia WB: Saunders Co; 1990. p. 652.
-
- Shimokawa Y, Okuda K, Kubo Y, et al. Serum glutamic, oxaloacetic transaminase/glutamic pyruvic transaminase ratios in hepatocellular carcinoma. Cancer. 1977;40:319–324. - PubMed
-
- Cohen JA, Kaplan MM. The SGOT/SGPT ratio-an indicator of alcoholic liver disease. Dig Dis Sci. 1979;24:835. - PubMed
-
- Lee HS, Kim YT, Jung HC, et al. Prospective, randomized, controlled trial with diphenyl-dimethyl-dicarboxylate in chronic active liver diseases: The effect on lowering serum alanine aminotransferase levels. Korean Journal of Medicine. 1991;41:172–178.
-
- Konttinen A, Murros J, Okada K, Salaspuro M, Somer H, Ra‘sa’nen J. A new cause of increased serum aspartate aminotransferase activity. Clin Chim Acta. 1978;84:145–147. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous