

The potential role of procalcitonin and interleukin 8 in the prediction of infected necrosis in acute pancreatitis
- PMID: 9462219
- PMCID: PMC1891610
- DOI: 10.1136/gut.41.6.832
The potential role of procalcitonin and interleukin 8 in the prediction of infected necrosis in acute pancreatitis
Abstract
Background: Infection of pancreatic necrosis has a major impact on clinical course, management, and outcome in acute pancreatitis. Currently, guided fine needle aspiration is the only means for an early and accurate diagnosis of infected necrosis. Procalcitonin (PCT), a 116 amino acid propeptide of calcitonin, and interleukin 8 (IL-8), a strong neutrophil activating cytokine, are markers of severe inflammation and sepsis.
Aims: To analyse the clinical value of PCT and IL-8 as biochemical parameters for predicting infected necrosis in acute pancreatitis.
Patients and methods: Fifty patients with acute pancreatitis entered this prospective study and were stratified into three groups according to morphological and bacteriological findings: 18 patients with oedematous pancreatitis (group I), 14 patients with sterile necrosis (group II), and 18 patients who developed infected necrosis a median of 13.5 days after the onset of symptoms (group III). After admission serum samples were drawn daily for two weeks. Concentrations of PCT and IL-8 were measured by chemoluminescent immunoassays (upper reference range 0.5 ng/ml for PCT and 70 pg/ml for IL-8). The routine parameter C-reactive protein was determined by laser nephelometry (upper reference range 10 mg/l).
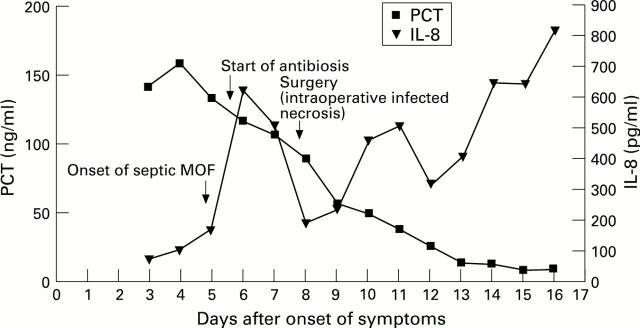
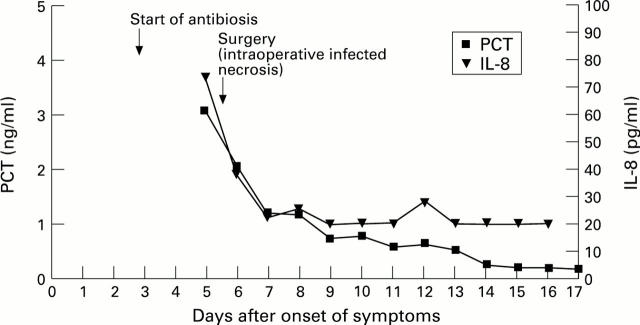
Results: Median concentrations of PCT and IL-8 were significantly higher in patients with infected necrosis than in those with sterile necrosis during the observation period, whereas there was no difference in C-reactive protein. In oedematous pancreatitis overall median concentrations of all three parameters were low. By receiver operating characteristics best cut off levels for predicting infected necrosis or persisting pancreatic sepsis were 1.8 ng/ml for PCT and 112 pg/ml for IL-8. If these cut off levels were reached on at least two days, sensitivity, specificity, and accuracy for the prediction of infected necrosis were 94%, 91%, and 92% for PCT and 72%, 75%, and 74% for IL-8, respectively. After surgical treatment of infected necrosis median PCT and IL-8 values continued to be significantly higher in patients with persisting pancreatic sepsis (n = 11) compared with those having an uneventful postoperative course (n = 7). For the preoperative differentiation between infected necrosis and sterile necrosis guided fine needle aspiration was performed in 24 patients with necrotising pancreatitis and reached a diagnostic accuracy of 84% compared with 87% for PCT, and 68% for IL-8. There was no correlation between the aetiology of acute pancreatitis or the extent of necrosis and PCT or IL-8.
Conclusion: PCT and IL-8 are found in high concentrations in infected necrosis and associated systemic complications in patients with acute pancreatitis. The course of PCT shows the closest correlation with the presence of infected necrosis. Monitoring of serum PCT is a potential new marker for the non-invasive and accurate prediction of infected necrosis as well as for the selection of patients with persisting septic complications after surgical debridement.
Figures







References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials