

The unenlarged lymph nodes of HIV-1-infected, asymptomatic patients with high CD4 T cell counts are sites for virus replication and CD4 T cell proliferation. The impact of highly active antiretroviral therapy
- PMID: 9500797
- PMCID: PMC2212181
- DOI: 10.1084/jem.187.6.949
The unenlarged lymph nodes of HIV-1-infected, asymptomatic patients with high CD4 T cell counts are sites for virus replication and CD4 T cell proliferation. The impact of highly active antiretroviral therapy
Abstract
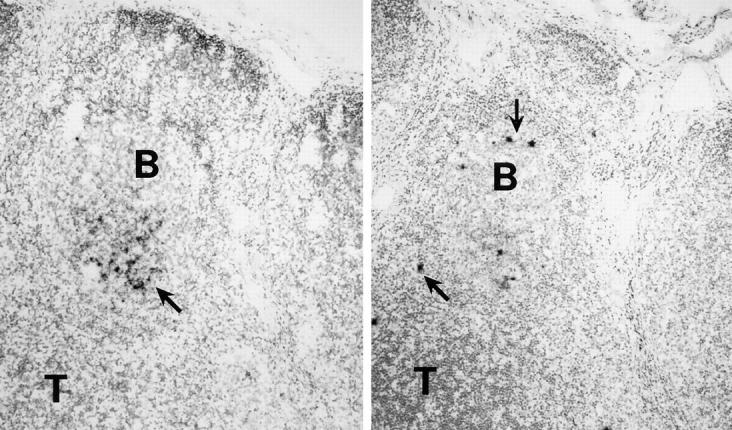
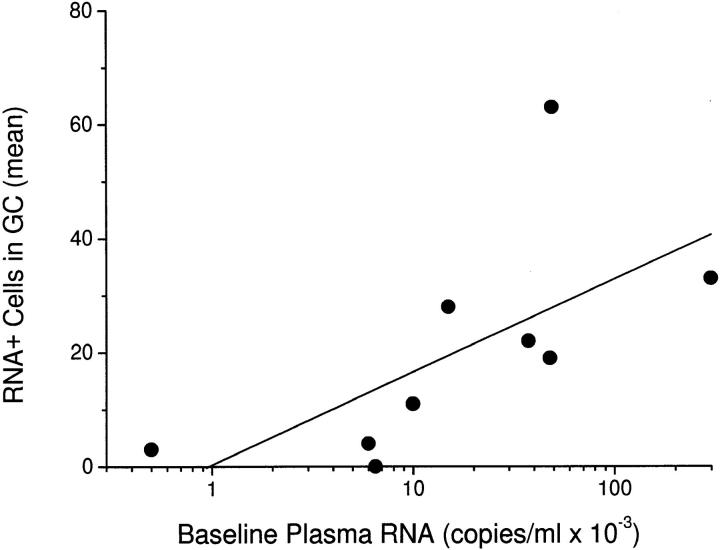
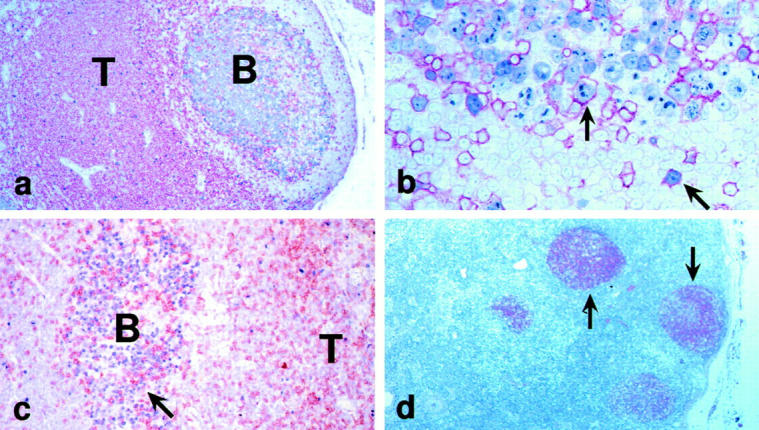
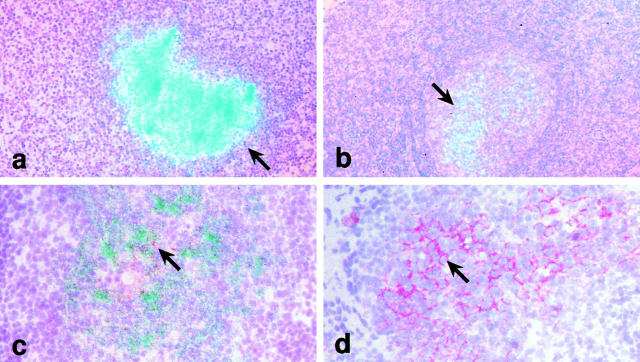
The efficacy of triple drug therapy for HIV-1 infection encourages its early use to prevent damage to the immune system. We monitored the effects of such therapy on 12 patients with 14-75-mo histories of minimal disease, i.e., CD4+ counts constantly >500/microl and little or no lymph node enlargement. In this way, we could first determine the extent of viral replication and immunoarchitectural changes in unenlarged nodes early in disease, and second follow the response to triple therapy in plasma and lymphoid tissue in tandem. As is known for lymph nodes with more advanced disease, the germinal centers showed productively infected T cells, i.e., CD4+CD1a-CD68- cells labeling intensely for HIV-1 RNA after in situ hybridization. The unenlarged nodes also showed extensive HIV-1 RNA retention on a well-preserved, follicular dendritic cell (FDC) network, and the follicles were abnormal. There were numerous CD8+ cells, many expressing TIA-1 granule antigen. Also, in contrast to normal follicles, CD4+ T cell proliferation was active, with marked increases in the number of cycling, Ki-67+CD4+CD45R0+ cells. After 28 d and 3 mo of therapy, productively infected T cells decreased dramatically and often were not apparent. The labeling of the FDC network for viral RNA also decreased, but not for gag protein. We conclude that HIV-1 replicates and accumulates in lymphoid organs before damage of the immune system, that at this stage of disease de novo production of T cells occurs in the lymphoid tissue, and that the infection is sensitive to triple drug therapy in both plasma and lymph nodes.
Figures
References
-
- Collier AC, Coombs RW, Schoenfeld DA, Bassett RL, Timpone J, Baruch A, Jones M, Facey K, Whitacre C, McAuliffe VJ, et al. Treatment of human immunodeficiency virus infection with sanquinavir, zidovudine, and zalcitabine. N Engl J Med. 1996;334:1011–1017. - PubMed
-
- Perelson AS, Neumann AU, Markowitz M, Leonard JM, Ho DD. HIV-1 dynamics in vivo: virion clearance rate, infected cell life span, and viral generation time. Science. 1996;271:1582–1586. - PubMed
-
- Tenner-Racz K, Racz P. Follicular dendritic cells initiate and maintain infection of the germinal centers by human immunodeficiency virus. Curr Top Microbiol Immunol. 1995;201:141–159. - PubMed
-
- Tenner-Racz K, Racz P, Schmidt H, Dietrich M, Kern P, Louie A, Gartner S, Popovic M. Immunohistochemical, electron microscopic and in situ hybridization evidence for the involvement of lymphatics in the spread of HIV-1. AIDS (Lond) 1988;2:299–309. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
