

Effectiveness of occlusion therapy in ametropic amblyopia: a pilot study
- PMID: 9505818
- PMCID: PMC1722055
- DOI: 10.1136/bjo.81.11.956
Effectiveness of occlusion therapy in ametropic amblyopia: a pilot study
Abstract
Aims/background: To examine the relative contributions of non-specific (for example, spectacle correction) and specific (that is, occlusion therapy) treatment effects on children with ametropic amblyopia. To assess the importance and practicality of objectively confirming the prescribed occlusion dose.
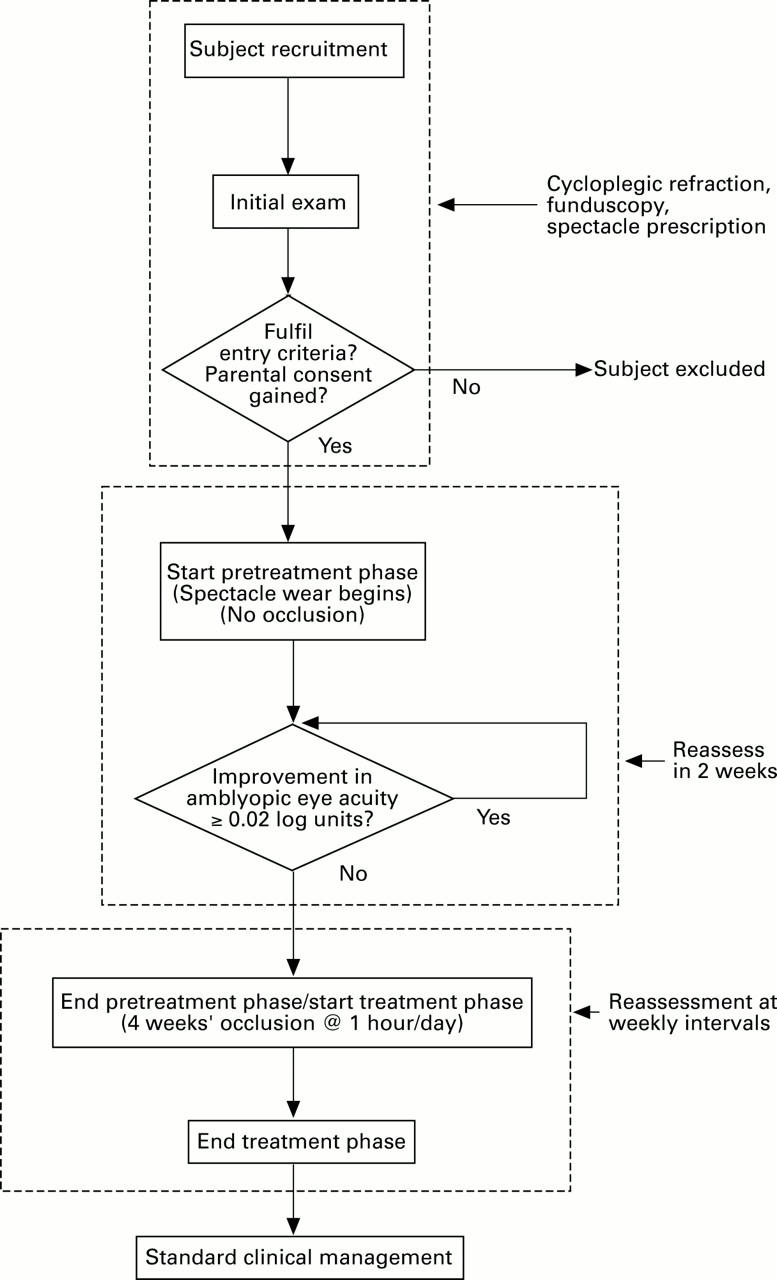
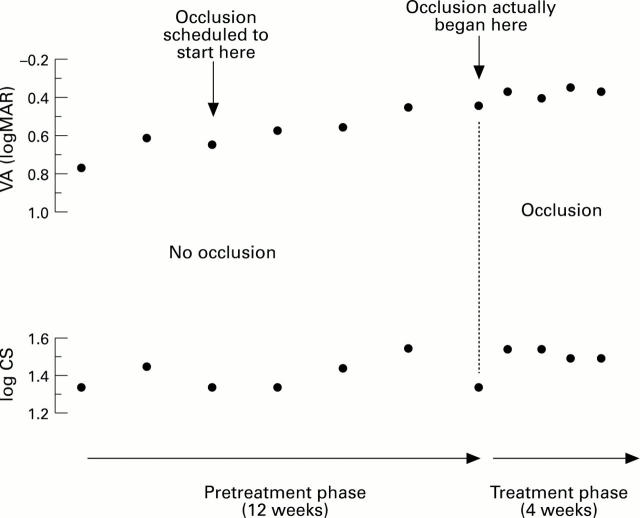
Methods: Subjects were entered into a two phase trial. In the first ('pretreatment') subjects were provided with spectacle correction and underwent repeat visual acuity (VA) and contrast sensitivity (CS) testing until acuity in their amblyopic eye had stabilised. Subjects then progressed to the second phase ('treatment') in which they underwent direct, unilateral occlusion for 1 hour per day for 4 weeks. Patching was objectively monitored using an occlusion dose monitor.
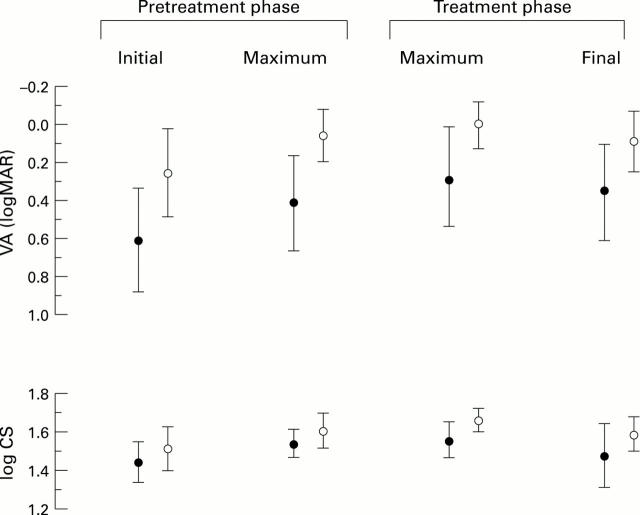
Results: Eight subjects completed the trial, all but one of whom achieved > 80% concordance with the occlusion regimen. Within the pretreatment phase, mean amblyopic eye VA improved by 0.19 log units (p = 0.008) while mean CS gained 0.09 log units (p = 0.01). An identical improvement in mean VA was recorded in the fellow eyes (p = 0.03) while mean CS gained 0.11 log units (p = 0.02). Within the treatment phase, mean VA further improved (0.12 log units, p = 0.009) although this gain had halved by the end of treatment and was no longer statistically significant (p = 0.09).
Conclusions: Visual performance improved significantly during pretreatment whereas further gains seen during occlusion were not sustained. Evaluation of occlusion regimens must take into consideration the potentially confounding influence of 'pretreatment effects' and the necessity to confirm objectively the occlusion dose a child receives.
Figures
Comment in
-
Effectiveness of occlusion therapy in ametropic amblyopia.Br J Ophthalmol. 1998 Jul;82(7):850. doi: 10.1136/bjo.82.7.849b. Br J Ophthalmol. 1998. PMID: 9924395 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical