

Clinical experiences of infectious scleral ulceration: a complication of pterygium operation
- PMID: 9505823
- PMCID: PMC1722042
- DOI: 10.1136/bjo.81.11.980
Clinical experiences of infectious scleral ulceration: a complication of pterygium operation
Abstract
Aims: To report the special clinical manifestations and determine the appropriate management of infectious scleral ulceration.
Methods: A retrospective study was performed on 30 eyes with infectious scleral ulceration. Information was recorded on patients' age, onset and course of disease, pathogenic organism, clinical presentations, methods of diagnosis, treatment, and outcome.
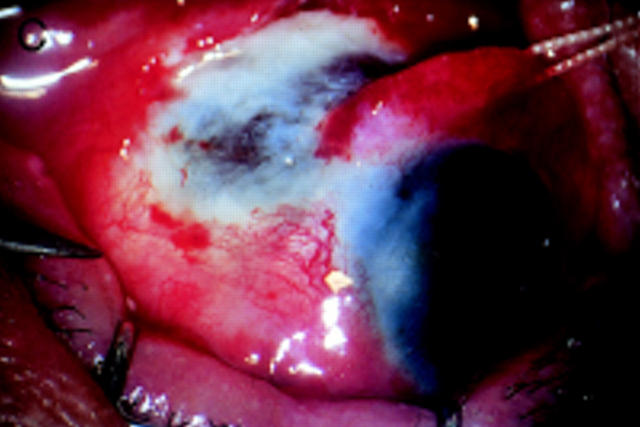
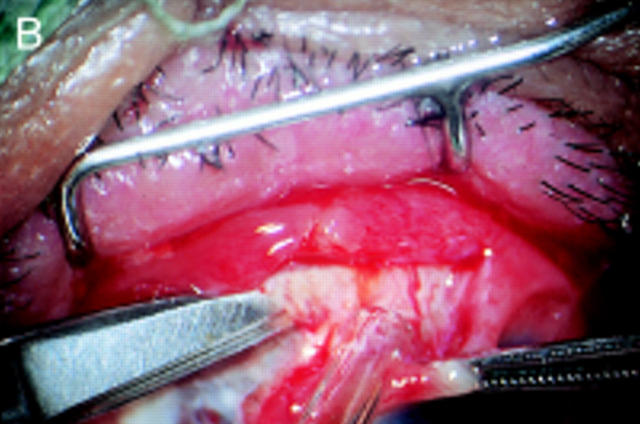
Results: 10 cases (33.3%) were accompanied by corneal involvement. Subconjunctival abscess was noted in 16 cases (53.3%). 17 cases (56.7%) gave positive results of pathogen culture and all were Pseudomonas aeruginosa. Two cases had combined bacterial infections and one case was complicated by fungal infection. A total of 26 cases had surgical debridement in this series. Extensive involvement of the sclera with the presence of a 'tunnel lesion' or a 'satellite subconjunctival abscess' were found during debridement. All of the eyeballs involved were salvaged except one.
Conclusion: The results of this study were contrary to the poor prognosis presented in previous reports. Early and repetitive surgical debridement is believed to be mandatory in the intractable cases to shorten the admission period and to save these eyes.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical