

Mathematical modeling of the interrelationship of CD4 lymphocyte count and viral load changes induced by the protease inhibitor indinavir
- PMID: 9527786
- PMCID: PMC105414
- DOI: 10.1128/AAC.42.2.358
Mathematical modeling of the interrelationship of CD4 lymphocyte count and viral load changes induced by the protease inhibitor indinavir
Abstract
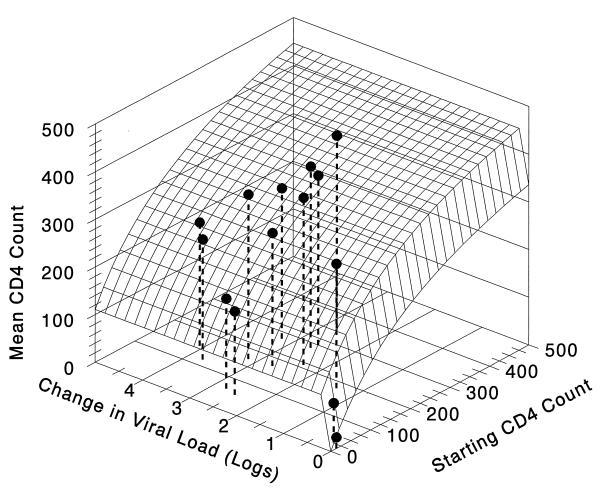
While CD4 cell counts are widely used to predict disease progression in human immunodeficiency virus (HIV)-infected patients, they are poorly explanatory of the progression to AIDS or death after the introduction of chemotherapy. Changes in HIV load (as measured by RNA PCR) have been shown to be a much better predictor of the risk of disease progression. Since the interrelationship of these markers is of great clinical interest, we modeled the time-averaged return of CD4 cell count and change in viral load subsequent to therapy with the HIV protease inhibitor indinavir. We found that CD4 cell return was significantly related to both the baseline CD4 count (r2 = 0.86, P < 0.001) and the decline in HIV RNA PCR-determined viral load (also referred to in this work as the HIV RNA PCR decline) (r2 = 0.60, P < 0.01). Simultaneously modeling both influences in a linked nonlinear model (r2 = 0.93, P < 0.001) demonstrated that (i) the starting number of CD4 cells accounted for the majority of the change in CD4 cell return and (ii) the return of CD4 cells attributable to viral load decrease was 50% of maximal with only a decrease of approximately 0.2 log of HIV RNA as modeled from the first 12 weeks of therapy. Much greater viral inhibition beyond that necessary for maximal CD4 cell return is possible. Given that HIV RNA PCR decline is more strongly linked to ultimate clinical course in HIV disease, our findings indicate that CD4 return is potentially misleading as an indicator of antiviral effect, since it is determined more by the starting CD4 value than by viral load decline and since near-maximal changes occur with minimal antiviral effect.
Figures
References
-
- Cavert W, Staskus K, Zupanic M, Wietgrefe S, Notermans D, Danner S, Henry K, Mills R, Haase A T. Abstracts of the 4th Conference on Retroviruses and Opportunistic Infections, Washington, D.C. 1997. Quantitative in situ hybridization measurement of HIV-1 RNA clearance kinetics from lymphoid tissue cellular compartments during triple drug therapy, abstr. LB9.
-
- Cohen O J, Pantaleo G, Holodniy M, Fox C H, Orenstein J M, Schnittman S, Niu M, Graziosi C, Pavlakis G N, Lalezari J, Bartlett J A, Steigbigel R T, Cohn J, Novak R, McMahon D, Bilello J, Fauci A S. Antiretroviral monotherapy in early stage human immunodeficiency virus disease has no detectable effect on virus load in peripheral blood and lymph nodes. J Infect Dis. 1996;173:849–856. - PubMed
-
- Collier A C, Bozzette S, Coombs R W, Causey D M, Schoenfeld D A, Spector S A, Petinelli C B, Daivies G, Richman D D, Leedom J M, Kidd P, Corey L. A pilot study of low-dose zidovudine in human immunodeficiency virus infection. N Engl J Med. 1990;323:1015–1021. - PubMed
-
- D’Argenio D Z, Schumitzky A. ADAPT II user’s guide: pharmacokinetic/pharmacodynamic systems analysis software. Los Angeles, Calif: Biomedical Simulations Resource; 1997.
-
- De Jong M D, Veenstra J, Stilianakis N I, Schuurman R, Lange J M A, DeBoer R J, Boucher C A B. Host-parasite dynamics and outgrowth of virus containing a single K70R amino acid change in reverse transcriptase are responsible for the loss of human immunodeficiency virus type 1 RNA load suppression by zidovudine. Proc Natl Acad Sci USA. 1996;93:5501–5506. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
