

Bone mineral density and nutritional status in children with chronic inflammatory bowel disease
- PMID: 9536942
- PMCID: PMC1726993
- DOI: 10.1136/gut.42.2.188
Bone mineral density and nutritional status in children with chronic inflammatory bowel disease
Abstract
Background: Osteoporosis has been reported in adult patients with inflammatory bowel disease.
Aims: To evaluate bone mineral density (BMD), nutritional status, and determinants of BMD in children with inflammatory bowel disease.
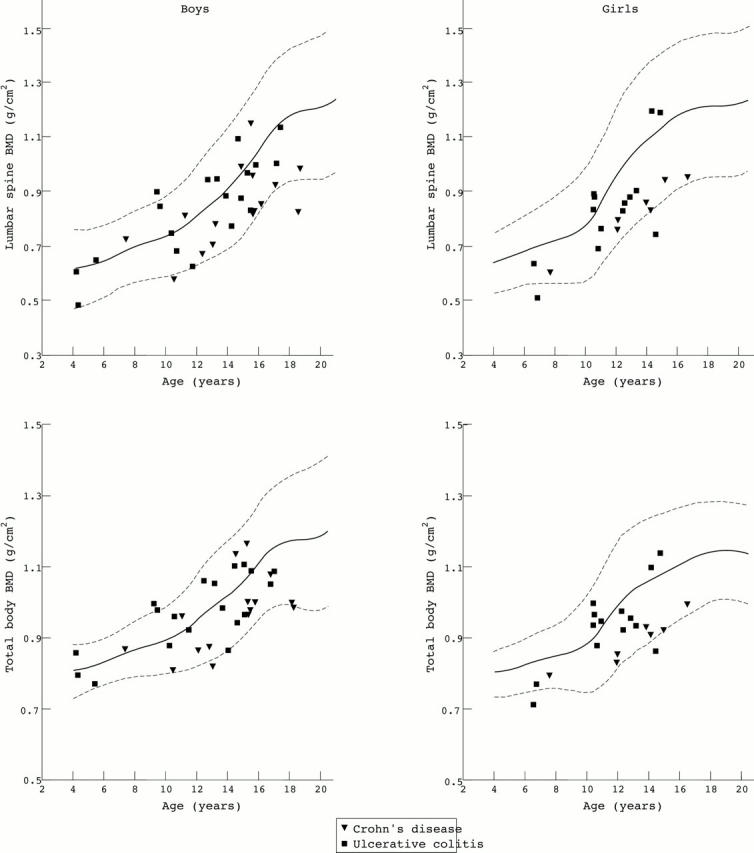
Patients: Fifty five patients (34 boys and 21 girls, age range 4-18) were studied; 22 had Crohn's disease and 33 ulcerative colitis.
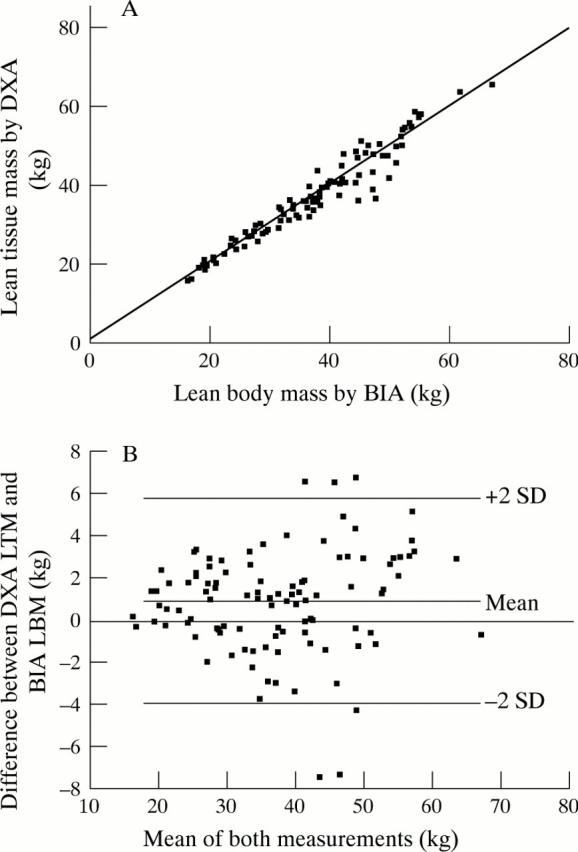
Methods: Lumbar spine and total body BMD, and body composition were assessed by dual energy x ray absorptiometry (DXA). Results were expressed as standard deviation scores (SDS). Lean body mass was also assessed by bioelectrical impedance analysis (BIA). Yearly measurements during two years were performed in 21 patients.
Results: The mean SDS of lumbar spine BMD and total body BMD were significantly lower than normal (-0.75 and -0.95, both p < 0.001). Height SDS and body mass index SDS were also decreased. The decrease in BMD SDS could not be explained by delay in bone maturation. The cumulative dose of prednisolone correlated negatively with lumbar spine BMD SDS (r = -0.32, p < 0.02). Body mass index SDS correlated positively with total body BMD SDS (r = 0.36, p < 0.02). Patients with Crohn's disease had significantly lower lumbar spine and total body BMD SDS than patients with ulcerative colitis, even after adjustment for cumulative dose of prednisolone. In the longitudinal data cumulative dose of prednisolone between the measurements correlated negatively with the change in lumbar spine and total body BMD SDS. Lean tissue mass measured by DXA had a strong correlation with lean body mass measured by BIA (r = 0.98).
Conclusions: Children with inflammatory bowel disease have a decreased BMD. Children with Crohn's disease have a higher risk of developing osteopaenia than children with ulcerative colitis. Corticosteroid therapy and nutritional status are important determinants of BMD in these patients.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical